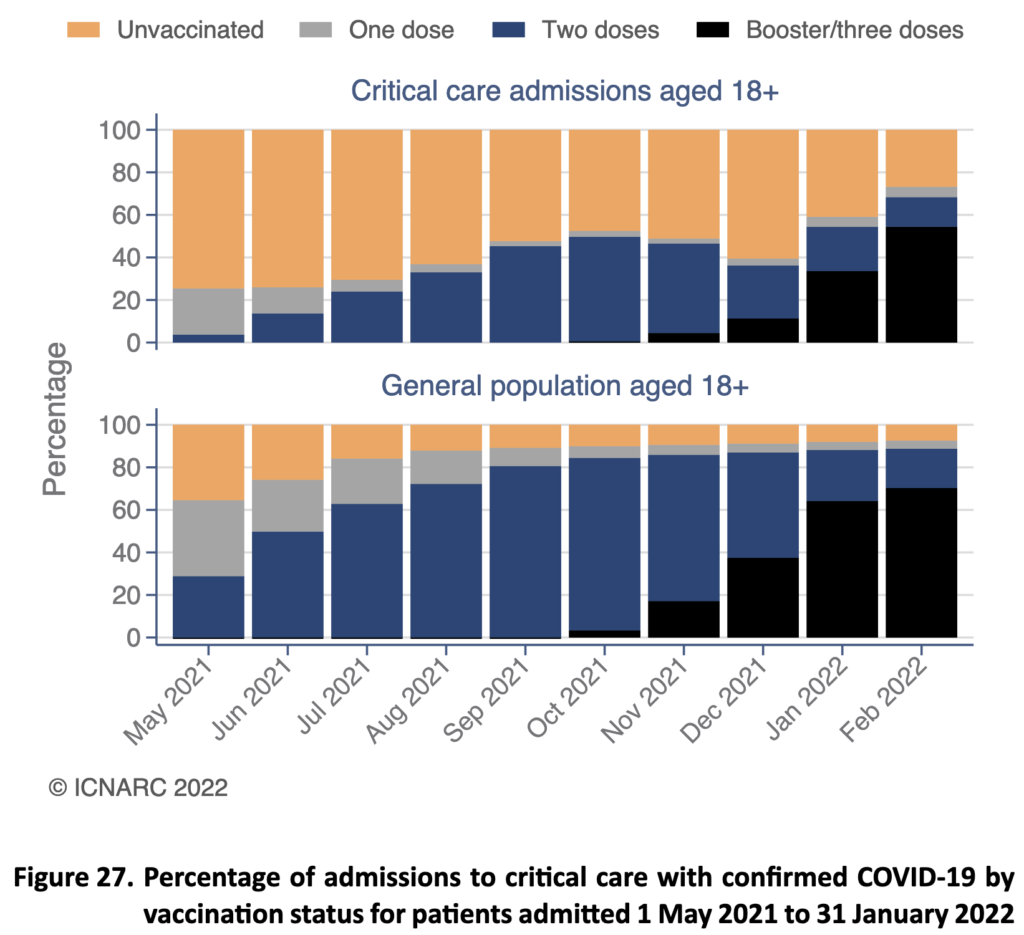
But this doesn’t mean the booster isn’t working at all because if an increasing number of people are triple jabbed then even if a small percentage get admitted it’ll be an increasing number of people as more get triple jabbed. Roughly, from the maths, this ICU data shows that a triple jabbed person is 2.5 times less likely to end up in ICU.
I prefer to consider the ICU data than the widely reported ‘deaths within 28 days of a positive covid test’, especially now when many people become infected but much more mildly. That will really crank up the false ‘covid’ death rate. For example, if you expect 100 deaths in an uninfected population, then everyone becomes infected and there’s 101 deaths, while it would count for ‘100 deaths with covid’ it would actually be 1 death from covid. The fact that weekly ICU deaths from covid have remained flat since Christmas makes this direction of bias in the numbers a likely scenario. One of my medical colleagues told me “We haven’t had a ‘real’ case in ICU for weeks.” Similarly, despite very high rates of infection, these aren’t leading to significant increases in hospitalisation.
So where is the compelling evidence that the third booster vaccine is saving lives? It comes from the Office of National Statistics who track ‘deaths involving covid’ which includes anyone dying who tests positive within 28 days. This data does consistently show lower mortality in those who’ve had the booster, compared to those who’ve had two vaccinations or the unvaccinated, each month since the booster started to be rolled out in November. Back in the autumn the risk of mortality of the unvaccinated and double-jabbed was equivalent, suggesting any vaccine benefit had worn off. Since then, those who’ve had the booster have consistently had lower mortality. However, even if a large portion of ‘deaths with a positive covid test’ are not actually deaths from covid it does appear those boosted have less risk of mortality overall.
In terms of studies we have one from Israel, who were the first to start vaccinating and have now given many a fourth vaccination, or second booster, comparing those vaccinated with a third booster and those with a fourth booster in people aged 60+. Broadly speaking those receiving the fourth booster were roughly half as likely to become infected and half as likely to suffer severe covid. They point out that ‘Protection against confirmed infection appeared short-lived, whereas protection against severe illness did not wane during the study period’ which was 8 weeks.
My view is we are now very in the same territory as a flu jab reducing severe infection and death by something like a half. Yes, the third booster saves some lives in the most vulnerable. Yes, it causes adverse effects, some long-term, in a minority. The benefits may last 3 months. It is thus moderately effective but not truly necessary for otherwise healthy people with good vitamin DWhat it does: Helps maintain strong and healthy bones by retaining calcium. Deficiency Signs: Joint pain or stiffness, backache, tooth decay, muscle cramps, hair loss…. status who know to take high dose vitamin CWhat it does: Strengthens immune system – fights infections. Makes collagen, keeping bones, skin and joints firm and strong. Antioxidant, detoxifying pollutants and protecting against… and zincWhat it does: Component of over 200 enzymes in the body, essential for growth, important for healing, controls hormones, aids ability to cope with stress… upon infection.
The main, but not only cause of concern regarding adverse effects is heart inflammation (carditis) and thrombocytopenia (clotting). In the UK yellow card reporting system there have been 2,099 cases of carditis reported as of March 23rd, eight of which were fatal. Not all will be due to vaccination but also the yellow card reporting system is estimated to represent one fifth of actual cases.
The risk/benefit equation still doesn’t stack up for teenagers and children, especially given the now established risk of carditis, which is highest in those under age 29, with 225 cases per million reported in the UK on the yellow card reporting system. This means 2.2 cases per 10,000, or if under-reported by a factor of 5, 1 case per thousand. These odds might seem small but they are a lot higher than the risk of critical or fatal covid in this age group, especially for those under 14. Deaths with covid (not from covid) in this age group is 15 which is 1 per 500,000.
As with any treatment one has to consider what else is on offer. Now that government health agencies have publicly listed all the 77 clinical trials of vitamin C and/or D for covid my request is that they actually review this evidence, and put these approaches alongside the benefit/risk equation for vaccination so people can make an informed choice about what to do, which could be both vaccination and vitamins, which may also reduce risk of vaccine adverse effects. I cannot envisage any analysis that would put ongoing vaccination ahead of a vitamin-based strategy for younger people.
Comments
Join the Conversation on our Facebook Page