More than 1 in 3 people now have a lifetime risk of developing cancer. Broadly, it is an overgrowth condition, and a communication breakdown at a cellular level. Cells are meant to behave and respect their neighbours. Cancer cells are healthy cells gone rogue because they weren’t getting the ‘love’ (nutrients or too many anti-nutrients) they needed to stay healthy. While using cancer killing ‘cytotoxic’ agents – natural or chemical eg chemotherapy is entirely appropriate, along with surgery if possible, you have to also address the toxic environment that allowed the cancer cell to develop and grow in the first place.
Most cancer cells are sugar hungry. Nobel Prize-winner, the German biochemist Otto Warburg, realised that cancer cells generate energy in a different way from healthy cells way back in the 1920s. Thereafter, further research established that the latter generate energy via their mitochondria, the energy factories inside cells. Essentially, healthy cells take glucose from the bloodstream and modify it into a substance known as pyruvate. This then travels through a channel in the mitochondria, where it is combined with oxygen – also drawn from the blood – to produce a chemical called ATP, which is the body’s main unit of energy. By contrast, cancer cells have little or no ability to generate energy via their mitochondria. (It’s not clear why this is the case, but it may have something to do with the fact that these cells undergo structural changes in the process of becoming cancerous.)
Instead, they generate their ATP directly from glucose, which is almost eighty times less efficient than generating it from pyruvate. As result, cancer cells need massive amounts of glucose. Indeed, this is why PET scans use radioactive glucose as a marker – it floods into the areas where cancerous tumours are growing. Anyone who uses PET scans to find tumours but denies that sugar has anything to do with cancer simply doesn’t understand why PET scans work.
A high fatThere are many different types of fats; polyunsaturated, monounsaturated, hydrogenated, saturated and trans fat. The body requires good fats (polyunsaturated and monounsaturated) in order to… ketogenic diet, as I’ve extolled in the Hybrid Diet , drastically reduces the amount of glucose in the bloodstream, then the mitochondria of healthy cells use ketones to generate ATP. However, crucially, cancer cells cannot convert ketones into ATP. So, in effect, the diet specifically targets cancer cells while allowing healthy cells to keep functioning normally. This is in sharp contrast to conventional chemotherapy, which targets all of the body’s fast- growing cells – healthy and cancerous alike – hence many of its unpleasant side- effects. Moreover, as it drastically reduces a tumour’s supply of fuel and therefore energy, the diet should make the cancer more vulnerable to chemotherapy. So, patients may need lower doses to achieve the same effect, and the side- effects should be less severe.
One promising and practical approach is to consume C8 oil, a subfraction of coconut oil, fromn which the body makes ketones. These ketones fuel all cells except cancer cells. Coupled with a very low carb diet one is effectively cutting off a cancer cell’s fuel supply.
Dr Nelofer Syed, Senior Research Fellow and Lecturer in Cancer Biology at Imperial College London, is just one of an increasing number of advocates of this theory: ‘Early research shows that the diet can improve the effectiveness of both chemotherapy and radiotherapy and that cancers find it difficult to use ketones for energy.’ Her research also suggests that the ketogenic diet can make it difficult for tumours to hook up to a local blood supply, reduce inflammation and make it harder for the cancer to spread.
In one paper, she and her colleagues conclude: ‘Emerging data provides strong support for the use of the ketogenic diet in the treatment of malignant gliomas [brain cancers]1.’
Dr Thomas Seyfried uses a ketogenic diet, plus supplements of HCA (garcinia cambogia) which is one of the ingredients in GL Support, in his patients with glioma brasin cancers and lung adenocarcinomas.
Personalisation is Key
We cannot assume, however, that a ketogenic diet is good for all types of cancer. Every cancer cell is different and that’s why personalization is so key.
So much has been learnt about cancer cells and genes in recent years that herald a fundamental shift in treatment, based on targeting the many stages of cancer growth and spread, and the many weaknesses of cancer cells. This new understanding, plus major developments in testing, is leading to a much more personalized and effective treatments.
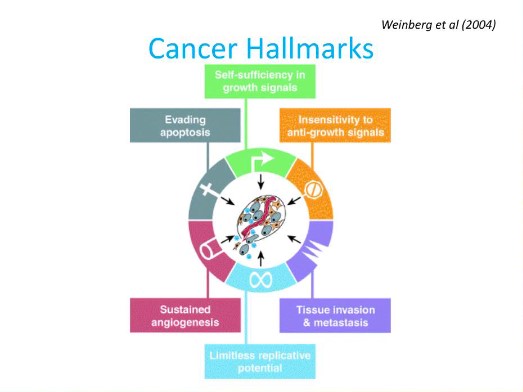
To understand how this works it is important to first understand what we know about cancer. Cancer cells have certain characteristics that make them different to normal cells. Unlike normal cells, which require ‘growth’ signals to grow – such as IGF-1, a hormone that goes up when you drink lots of milk – cancer cells grow of their own accord, and they can also replicate. They are also insensitive to anti-growth signals. They also encourage blood vessels to grow into them and feed them with nutrients. This is called angiogenesis and akin to taking over the transport system. They also invade surrounding tissue and send out satellite cancer cells that produce secondary tumors. This is called metastasis, which is what kills, much more than primary tumors.
The old view of cancer proposed that DNA in the nucleus of a cell gets damaged and the cell becomes a cancer cell, then replicates producing ‘clone’ cancer cells with the same gene damage of variations. Now that it is possible to ‘gene sequence’ DNA within cells very rapidly and inexpensively, what has become clear is that there are virtual no two identical cells within a primary tumor, no clone type of cell, which invalidates the ‘gene’ model.
The classic experiment that blew the ‘gene theory’ found that inserting the nucleus of cancer cells into the cytoplasm of healthy cells, and transplanting into animals (think of the nucleus as the yolk, and the cytoplasm as the white) only resulted in cancer in 17% of animals, but inserting a healthy nucleus into a cancer cells cytoplasm, and transplanting that, resulted in cancer in 97%!
Proteins ‘read’ DNA, which is a set of instructions held in the spirally chromosome. This DNA code is the cell’s blueprint, which is then copied as RNA to transfer to a new cell. The RNA then creates the DNA in a new cell. The body’s proteins are made from reading the RNA and DNA. We now know that damage occurs to the RNA, as well as the DNA, and to the proteins that ‘read’ RNA and DNA, and also to the resulting proteins made from the RNA and DNA.
What we also know is that cancer cells are changing (mutating) all the time and what primary cancer cells and secondary cancer cells respond to is not the same. There are several kinds of cells within a tumor, but very few can migrate into the bloodstream and thus trigger secondary tumors. These are therefore called Circulating Tumor Cells, or CTCs for short.
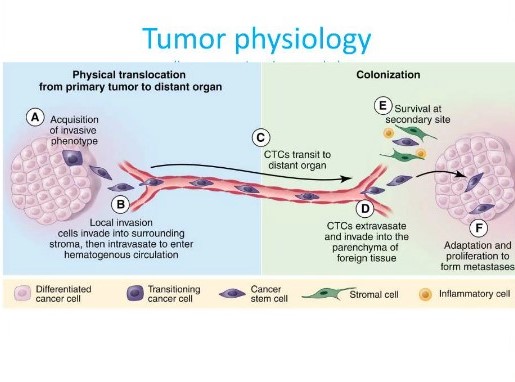
So, if you want to find out the specific characteristics of a cancer cell to target with specific drugs or natural agents it is better to analyse the CTCs rather than the primary tumour. Targetting CTC’s unique characteristics is proving much more effective and the level of CTCs is a good predictor of whether a treatment is working, according to a recent study of lung cancer.
For example, you can have a estrogen positive primary tumor and a non-estrogen positive secondary or CTCs. If a agent that blocks estrogen receptors were given (such as Tamoxifen or Genistein in soya) this would not be effective in inhibiting the formation of secondaries, even though it might suppress growth of the primary tumor.
The existent of advanced tests that can tell you all this, such as RGCC’s Onconomics is not only personalizing and vastly improving cancer treatment but also enables one to test the presence of CTCs which would not show up with a PET or MRI scan or biopsy.
The Stages of Cancer
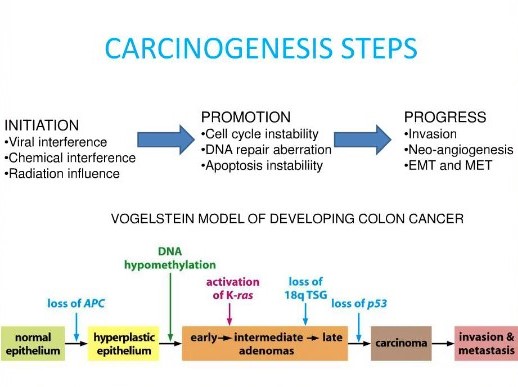
As I wrote about in my Say No to Cancer book there are three stages of cancer:
- Initiation – things that start to turn a cell into a cancer cell
- Promotion – situations and substances that make cancer cells grow
- Progress to invasion – at which point a cell becomes immortal and able to migrate, producing secondaries.
Although not a stage, since it can effect every stage, there is a fourth part which is boosting the body’s own natural immunity. More than anything, what has been learnt about cancer is that it is the environment that cells are exposed to that can initiate cancer. In the 19th century, Claude Bernard and Antoine Bechamp had proposed that it was the environment, or terrain, of cells that was key to them staying healthy and ‘uninfected’. While Louis Pasteur got much of the credit for his focus on germs, on his deathbed he is reported as saying “Bernard was correct. I was wrong. The microbe (germ) is nothing. The terrain (milieu) is everything.” Optimum nutrition has a massive effect on boosting immunity, while several chemotherapy drugs, as well as radiation are immune depleting.
Now, the reality is that old fashioned standard cancer treatment is remarkably ineffective. In a study of 154,971 Americans and Australians with cancer, age 20 and older, that were treated with conventional treatments, including chemotherapy only 3,306 had survival that could be credited to chemotherapy. The researchers concluded ‘The overall contribution of curative and adjuvant cytotoxic chemotherapy to 5-year survival in adults was estimated to be 2.3% in Australia and 2.1 % in The USA.’ While overall success of conventional cancer treatment (chemotherapy, radiation and surgery) in actually curing cancer averages 5 to 7.5%.
Chemosensitvity Testing
A test like RGGC’s Onconomics which is also called a ‘chemosensitivity’ test, but identifying the exact characteristics of CTCs, can allow an oncologist to give targeted compounds or treatment, be they natural or pharmaceutical, that work specifically on one of these characteristics. The trouble is very few are using this kind of personalized testing. It is also quite expensive – around £2,000 for a full test of all drugs and natural agents.
By looking at the genes that are activated (expressed) in the CTCs it is possible to know whether to target reducing growth signals such as IGF-1, or to inhibit angiogenesis, or whether there’s a methylationMethylation is what occurs when the body takes one substance and turns it into another, so that it can be detoxified and excreted from the… problem, or whether the cancer cell would be responsive or resistant to heat therapy (hyperthermia) or radiation. This is by no means a comprehensive list of all that can be learnt by looking close up on the gene expression of cancer cells but serves as an example. That’s the theory.
But what a chemosensitivity test does is to actually expose these cancer cells to agents – both drugs and natural agents – to see to what extent they do actually suppress growth or kill the cancer cell. That’s the ‘practice – at least at a cancer cell level in a test-tube.
Armed with this knowledge you actually want a three-pronged attack with treatments that are either:
1 directly cytotoxic, that is they kills cancer cells (eg Artemesia, vitamin CWhat it does: Strengthens immune system – fights infections. Makes collagen, keeping bones, skin and joints firm and strong. Antioxidant, detoxifying pollutants and protecting against… etc)
2. or inhibit a growth factor (quercetin, curcumin from turmeric – has a quinazoline structure)
3. or stimulate the immune system against the cancer cell (Mistletoe – lectins)
A chemosensitivity test tells you which agents – both drugs and naturals – are likely to work and grades them in % effective. You ideally want something that is 70% or more effective, and not below 30%.
Oncologists find this really useful. The last two patients I was asked to advise re their nutrition had RGCC tests that confirmed that the chemo drug chosen by their oncologist was the best against their specific tumour, but it also identified other drugs, and natural agents, that would be highly effective.
It doesn’t, however, directly compare the drugs with the naturals. This is difficult to do at this stage because there is a lot of variation in the form of natural agents and doses given. For example, curcumin from turmeric is one of the most commonly effective natural agents. But it is very poorly absorbed so the supplement you choice, and the dose, is very important. Theracurmin is one of the most absorbable forms. Also, a lot of natural agents degrade very quickly so you need to take them frequently, and at relatively high doses. Also, a factor to consider is the toxicity, or adverse effects of drug versus natural agents. Some drug treatments have severe adverse effects and the patient’s resilience and immunity can be severely compromised. Natural agents generally come out much better in this respect. Some also mitigate the adverse effects of the drugs or radiation treatment. For example, high dose vitamin C has been shown to both render some chemotherapy agents less toxic, and enhance their efficacy, which means, theoretically, a lower dose can be given. It is also likely that vitamin C, given concurrently with radiotherapy, makes it more effective, based on animal studies. This is obviously a ‘win-win’ but it is hard to find oncologists will to deliver both treatments since few are sufficiently informed about natural cancer therapies. Vitamin C is both cytotoxic and immune boosting so it ticks two boxes. Ideally you want both intravenous vitamin C and high oral doses. Vitamin C and curcumin are two of the most common natural agents to come up trumps in chemosensitivity testing but my past client’s results showed that vitamin C would not be effective for her.
Many drugs are very similar to natural agents and once you know what the drug or natural agent is targeting it is hard to dismiss natural agents. For example, a lot of chemotherapy drugs designed to inhibit cancer cell growth do so because they contain a chemical structure called a quinazoline ring which fits into proteins inside cancer cells and stops them growing. Both quercetin (in red onions) and curcumin (in turmeric) contain a quinazoline ring and are thus chemotherapy agents.
Some drugs block growth by blocking estrogen receptors. Tamoxifen is an example. But genistein, a phytoestrogen from soya, does. Also, indole-3-carbonol, rich in broccoli, helps to detoxify and breakdown excess oestrogenOestrogen is one of the main female sex hormones…., thus inhibiting growth of estrogen-positive cancer cells. This would be very relevant for most cases of breast cancer. The combination would be effectively tackling the issue on all sides. Some women are also given a forced menopause to strop oestrogen production for a period of time.
Other drugs are ‘cytotoxic’ meaning they are designed to kill cancer cells. Quite a few of these drugs work through a pro-oxidant effect. Vitamin C, in high doses, acts as a pro-oxidant within cancer cells, but not in healthy cells. So too does the herb Artemisia Annua (sweet wormwood) and its extract Artemesinin. This is thought to be because cancer cells accumulate, and need ironWhat it does: As a component of red blood cells, iron transports oxygen and carbon dioxide to and from cells. Also vital for energy production….. When in contact with iron both vitamin C and artemisinin produce free oxidizing radicals which damage and hopefully kill the cancer cell.
Very few drugs boost immunity while vitamins A, C and D (which can also be cytotoxic in high doses) do. One of the most effective herbs for stimulating the immune system to attack cancer cells is Mistletoe.
Whether a patient/doctor team chooses to use drugs and/or natural agents the goal is to target all three areas to give cancer cells a hard time. Also, since cancer cells are notoriously adaptive, it is sometimes good to change the treatment every 3 or so months so the cancer cells don’t become resistant to the drug or natural agent. However, the good thing about chemosensitivity testing is that you can retest the level of circulating tumour cells and if they’ve come down a lot on a particularly strategy, stick with it and, if not, move on to a new set of agents.
If you’d like to find a doctor using chemosensitivity testing either email info@rgcc-europe-nw.com who can provide you with a list of doctors in the UK and put you in touch with others if you live abroad or visit www.rgcc-europe-nw.com
Further Information
To dig deeper into natural ways to reduce your risk read Say No to Cancer. Theracurmin, high potency ImmuneC powder, Ketofast (pure C8 oil) GL Support (containing HCA from garcinia cambogia) are available from www.holfordnutrition.com.
References
1. 1. E.C. Woolf et al., ‘Tumor metabolism, the ketogenic diet and β-hydroxybutyrate: novel approaches to adjuvant brain tumor therapy’, Frontiers in Molecular Neuroscience, vol 9:122;
also see A. Poff et al., ‘Targeting the Warburg effect for cancer treatment: ketogenic diets for management of glioma’
also see K.J. Martin-McGill et al., ‘The modified ketogenic diet in adults with glioblastoma: an evaluation of feasibility and deliverability within the National Health Service’, Nutrition and Cancer (2018), vol 70(4):643–649
Comments
Join the Conversation on our Facebook Page