Done in an organised way, a serious campaign to strengthen our immune systems with nutrition by tackling deficiencies would bring down the rate of serious infection, speeding up progress towards Level I. What might have happened to the early spike in infections had the Government rapidly copied the preventative actions taken in Wuhan, when 50 tons of vitamin CWhat it does: Strengthens immune system – fights infections. Makes collagen, keeping bones, skin and joints firm and strong. Antioxidant, detoxifying pollutants and protecting against… was shipped in and given to all health workers and patients?
Half of deaths happen in nursing homes
An estimated half of all Covid-19 deaths have happened in nursing homes, says the Guardian, where elderly patients have long been known to have weakened immune systems, Just looking after this ‘at risk’ group could have cut the numbers needing intensive care and substantially reduced the burden on the NHS.
Surprisingly perhaps, paying attention to nutrition would also be good for the pharmaceutical industry since vaccines work by triggering an immune response, mobilising the army of defensive cells to go on the attack.
Once you have been vaccinated, it is still left to the immune system to do the heavy lifting. Healthy immune cells can have several times the level of vitamin C in the blood, keeping them in a state of readiness. Patients with immune systems weakened by multiple deficiencies, mount correspondingly feeble responses, making vaccination far less effective.
Prevention is better than cure
The prevention strategies that should have employed include giving all NHS workers sufficient vitamin C, D and zincWhat it does: Component of over 200 enzymes in the body, essential for growth, important for healing, controls hormones, aids ability to cope with stress… support and doing the same in care homes. Once admitted to intensive care patients should get high doses of intravenous vitamin C. Most importantly people with symptoms would be told by the Government to take high doses of vitamin C – 8 or more grams per day. In the longer term a campaign to tackle metabolic diseases of obesity, diabetes and heart disease with diet and lifestyle is needed.
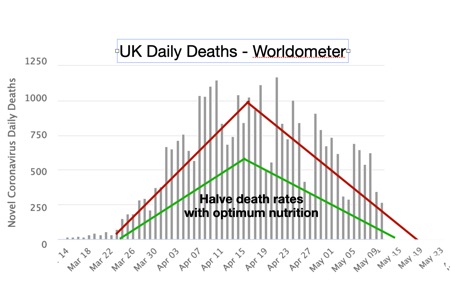
These initiatives could reasonably be assumed to halve current death rate. Yet advice to take several grams of vitamin C when the first symptoms start has been actively discouraged in almost all BBC coverage. The monthly cost of implementing this protocol would be less than the cost of a single ventilator. The two thirds mortality rate of patients in the UK on ventilators is substantially higher than that in intensive care units in America where an increasing number of hospitals are giving high dose vitamin C following reports of zero deaths.
Level 3 – R below 1
None of this is part of Boris’s battle plan to counter the virus. Instead it depends on a slowing in the rate of infections to be matched by a relaxing of lockdown. This is what is now happening, along with a drop in the death rate. In fact, we are heading rapidly for Level 3 with more returning to work. Level 3 is defined as a R value below 1 yet already the R value is between 0.5 and 0.9 depending on where you live. (The R value is the number of people someone infected with the virus will infect.) See the graph below, which indicates the death rate will be below 200 within a fortnight. So, have we got it cracked and will we soon be home free?
Not quite, or rather not at all. There are speed bumps ahead, several of them created by the vaccine strategy along with the Government’s rugged determination to ignore nutrition. In theory ‘partial lockdown’, the proposed action for Level 3, should relate only to those at high risk, which means anyone with diabetes, heart disease, hypertensionHypertension is more commonly known as high blood pressure…., low vitamin DWhat it does: Helps maintain strong and healthy bones by retaining calcium. Deficiency Signs: Joint pain or stiffness, backache, tooth decay, muscle cramps, hair loss…. levels, obesity and other immune compromising conditions, many of whom will be in care homes.
The conventional medical approach has very little to offer to protect the vulnerable from infection other than extended and cripplingly expensive lockdown. This targeted ‘high risk’ group could, on the other hand, be so easily supported with optimum nutrition.
Herd immunity
Which brings us to the strategy of ‘herd immunity’, not mentioned so much recently, but the very core of the spending of multiple billions on vaccine development.
Herd immunity is how flu epidemics end. It happens when a significant number of people become infected, developing antibodyAn antibody is a protein produced by the body’s immune system when it detects a harmful substance known as an antigen. Examples of antigens include… protection. It isn’t clear what percentage of the population is needed to become antibody positive to extinguish the virus, nor how many are already antibody positive. The results of surveys are always elusively a couple of weeks away and figures of between 20 and 60% are quoted. A quarter of people in New York and Stockholm, for example, are said to be antibody positive. Sweden went for herd immunity from the beginning, allowing low risk people to socialise, some of whom will suffer from infection, but not in a life threatening way, but isolating those at high risk, to speed up natural herd immunity.
Whatever the percentage of antibody protection then, when a vaccine arrives, it could protect the rest and the virus would have been defeated. That’s the Government’s plan. Of course, the big assumption here is that an effective vaccine will arrive in time and that this is the right approach. Boris’s definition of the journey’s end, Level 1 (green) depends on it: ‘‘For our lives to return to normal, we would need no transmission of infections in England. This situation is currently only foreseen in the event of a successful vaccine being administered across the country. Oxford University hopes to have a vaccine ready by as early as September.”
This is science fiction on three counts. Firstly, no vaccine, even one that arrived in a miraculous flash in September, could go through proper safety and efficacy checks in under two years. Secondly, no flu vaccination is 100% effective. Thirdly, zero deaths is an unrealistic target. It doesn’t happen with other flus – the UK’s average mortality rate from flu is 40 deaths a day, yet that doesn’t trigger lockdown. If zero deaths is the criterion for level 1 we’ll never be out of lockdown.
First do no harm
Any new treatment, including a vaccine, needs a placebo-controlled trial (none are currently underway or planned), which should be repeated by a research group with no commercial interest in it. A placebo is an inert substance such as sterile water, not another vaccine or aluminium containing vaccine mix without the ‘virus’ part.
Then there is the ethical hurdle of infecting healthy volunteers with the virus to check that the vaccine can protect them. Alternatively, the drug company can vaccinate a larger number of people, wait to see how many become infected and observe what happens to them. Maybe none of them develop symptoms, a few do, or the infection rate, severity and mortality is little better than the placebo group. Some may even get sick from the vaccine. We’ll have to wait and see. That’s why you have to do a placebo controlled trial.
Then the vaccinated volunteers must be monitored for side-effects for months, if not up to 2 years. That is because it’s well known that side-effects only clearly come to light after at least a year. Adverse effects from vaccines are very relevant although too often denied.
It is of course possible, actually very likely, that in the panic of a pandemic the push to get something, anything out there for both commercial and political reasons will be so strong that such red tape will be consigned to a bonfire.
According to Professor Sarah Gilbert, leading the study at Oxford University “if the vaccine proves to be successful then the team will apply for ‘emergency use approval’ to roll out the inoculation programme immediately.” The implication is that there will be casualties. It is also likely that those who warn about such side-effects will be dismissed as‘anti-vaxxers’. It is also likely that such a vaccine would be recommended, if not mandated, for all, without bothering to test for antibody positivity. Natural immunity is always more effective than a vaccine but no doubt the vaccine lobby will generate fear that one can become re-infected despite being antibody positive. If so, of course, the same applies to vaccines. From a business point of view an annual mandatory vaccine generates the most sales. (I’ll be posting a blog on antibody tests, and which ones work best, next week.)
No flu vaccine has been more than 50% effective
Secondly, there’s the illusion of an 100% effective vaccine. No flu vaccines have ever conferred more than 50% protection. In 2017/18 the flu jab was only 12% effective in those aged 18 to 64 and 10% effective in those aged 60 plus. In 2018/19 it was much better being 24% effective against H3N2 flu and 67% effective against H1N1 flu, averaging out at 50% effective. That still means half of those vaccinated would become infected and those with poor immune systems might die. Viruses are forever mutating. We’ve had eleven serious viral epidemics this century already. There will be more. The viruses can mutate much faster than we can develop vaccines. That’s why strengthening your natural immunity makes more sense.
Thirdly, zero mortality is a high bar, although I think it could be achieved with intravenous vitamin C. Regardless of covid-19 the average death rate from flu is 40 a day.
DefinE risk and act accordingly
What I’d like to see is a careful gathering of information about what is different between those who become antibody positive with either no or minor symptoms, and those who suffer severely and even die. Then we can define who is at ‘high risk’ and protect them. This ‘high risk’ group is likely to be older people with a poor immune system, or those with metabolic disorders such as diabetes, heart disease or obesity, or those clearly vitamin D deficient – a blood level of below 30nmol/l and possibly low vitamin C and zinc to boot. A good way to do this is to develop, and test, a ‘coronoa risk index’.
For example,
1. Low vitamin D (below 30nmol/l)
2. Diabetes
3. Hypertension/heart disease
4. Low fruit & veg intake (below 3 servings) and not supplementing vitamin C
5. Age ( 65+)
Score 1 if you answer ‘yes’. What’s the risk of death from covid-19 for those scoring 5 or 4 versus those score 1 or 0. That’s how you tease out those at risk and then have a public health campaign to reduce it. This information exists, right now, in the NHS database. This kind of study could be done in a fortnight.
Let’s assume two thirds of deaths are in the high risk groups – I suspect it will be more. Then, that would mean, right now, that the number of deaths in the vast majority of the population, those at low risk, is already below 100 a day and expected to be around 40 a day within two weeks. That’s equivalent to the average daily rate for flu deaths. (Of course, if the most effective ICU treatment of giving 12 grams of intravenous vitamin C plus steroids, were being used in the UK, even this could be lowered.)
That would mean that those in low risk groups are already in the green, at Level 1, with no real risk of dying. And that’s without a vaccine.
See Flufighters.net for podcasts, films and supporting information.
If you’d like to train in nutritional therapy the Institute for Optimum Nutrition (ION) offer an excellent BSC Hons course; or if are a health professional and would like a higher award in nutritional therapy visit ion.ac.uk.
Comments
Join the Conversation on our Facebook Page