COVID – Assess Your Risk
What is it that makes some people have a mild covid infection, similar to a cold and others suffer severely? Is it possible to work out your risk and, if high, what you need to do to prevent a severe covid infection if you become infected? What has become clear is that covid is not indiscriminate. Severe infection strikes men much more commonly than women. Black more than white. Those with pre-existing health conditions – diabetes, high blood pressure or COPD (chronic obstructive pulmonary disorder). Blood type A more than O and certain genetic types (called polymorphisms). Risk increases exponentially with age and also with degrees of material deprivation.
But what exactly is it about being male, darker in skin, diabetic, hypertensive and older or more materially deprived or genetically susceptible that makes your risk higher?
A new and comprehensive study attributes much of this increased risk to differences in blood levels of vitamin CWhat it does: Strengthens immune system – fights infections. Makes collagen, keeping bones, skin and joints firm and strong. Antioxidant, detoxifying pollutants and protecting against…. But not due to less dietary intake but more to do with differences in the rate of absorption of vitamin C, controlled by vitamin C transporters. These carry vitamin C from the gut into the bloodstream. Due to its water-soluble nature, and the gut wall having a layer of fatty membranes most vitamin C is actively carried across the gut wall and past these fatty membranes using a ‘fast track’ and ‘slow track’ sodium-dependent vitamin C transporter called SVCT 1 and 2.
What Professor Gregory Patterson and colleagues at the faculty of Medicine and Center for Healthy Ageing at Augusta University, Augusta, Georgia USA have found is a direct correlation between blood vitamin C level across all these characteristics that increase risk and relative chances of getting severe covid infection. 1
And it wasn’t just that men eat less than women. “In almost all studies, there was a statistically significant difference in average plasma vitamin C concentration between males and females, with male plasma vitamin C levels much lower than in females despite a diet consisting of higher levels of vitamin C”, says Patterson. The same, by the way, occurs with some other nutrients such as omega-3, perhaps as an evolutionary adaptation to protect the all-important potential mother and hence the survival of the species.
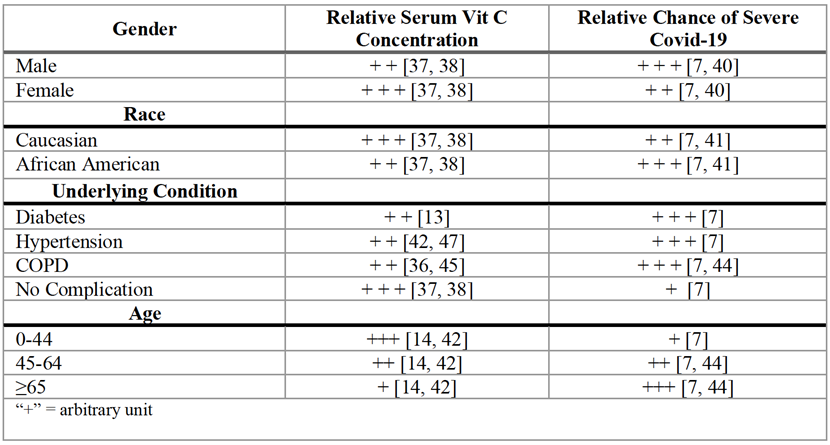
Used with permission of Patterson G et al, Aging and Disease 12 (2), April 2021
Could it be that the reason older versus younger, male versus female and black versus white people have a relatively higher risk is substantially to do with vitamin C absorption of intake? One tends to think that those with darker skin, and living up North, would be more likely to have lower vitamin DWhat it does: Helps maintain strong and healthy bones by retaining calcium. Deficiency Signs: Joint pain or stiffness, backache, tooth decay, muscle cramps, hair loss…., and it is broadly speaking true.
But what’s interesting is that in one Intensive Care Unit where they measured both vitamin C and D levels, while most of their critical covid patients had both low vitamin C and D. it was the vitamin C level that predicted survival2.
The average vitamin D level was not different between survivors and non-survivors. They also found that it wasn’t so much age that determined risk of death but actually the person’s vitamin C levels. The older the person the lower their vitamin C level was.3 This is probably less a function of a difference in diet and more in transportation.
Another classic predictor of mortality is the index of material deprivation with those in the highest fifth (quintile) for deprivation on the IMD scale having the greatest risk for mortality. But what is it about deprivation that leads to mortality?
Bear in mind that there may be many factors that lead to a greater risk of becoming infected and ending up in an ICU – from overcrowding to low vitamin D – but once in an ICU the critical question is what determines who will survive?
Deprivation, while a risk factor for COVID-19 mortality, is also a predictor of low vitamin C status. In the UK an estimated 25% of men and 16% of women in the low-income/materially deprived population are overt deficient with scurvy levels of vitamin C below 11 µmol/l. 4 .
What Paterson and colleagues point out is that “there are several in vitro and animal studies demonstrating drastically altered expression of vitamin C transporter mechanisms (SVCT1 and SVCT2) in the presence of oxidative stress, inflammatory factors, and various disease conditions such as diabetes.”
The Genetic Factor
Two areas of research have identified genetic predispositions that are associated with higher risk. Being blood type A is associated with more covid infection than being blood type O. In one study 57% of covid patients were blood type A compared to 24.8% being blood type O, thus doubling risk.5 This association has been confirmed by two other studies 6, also showing a higher rate of testing positive in those RH+ blood types. One study found that this association to blood type could not be explained by other risk factors such as age, sex and concurrent diseases. 7 While being blood type A and RH+ seems to increase risk of having covid infection, these studies do not show that, once infected, there is an increased risk of death.
The stronger association relates to a staggering discovery that 10% of severe covid patients produce ‘auto-antibodies’ that attack the body’s immune system much like an auto-immune disease. This discovery, was made by Jean-Laurent Casanova and his team at Rockefeller University. 8 At the time they had access to 1,500 severe covid patients and were sequencing their genes for clues as to what might make them different. They found that 23 out of 659 had errors in genes that make interferons. When a cell becomes virally infected it produces interferons to inhibit the virus’s ability to replicate so interferons are a vital part of our immune system’s self-preservation. They then found that 101 out of 987 were making auto-immune antibodies that inhibited interferon production.
While there is much yet to unravel it suggests that some people are more genetically suspectible and that a big part of that suspectibility lies in reduced interferon production as a consequence of auto-immunity. Interferon production is dependent on vitamin C. While the covid virus downregulates the activity of interferons, vitamin C upregulates this key anti-viral protection mechanism 9. In GULO knockout mice, who have lost the GULO enzyme that makes vitamin C – just like us – giving vitamin C improves anti-viral immune responses at the start of infection, especially against flu viruses, through increased production of interferon.10
What all this implies is that it doesn’t matter whether you are old, male, black, diabetic or blood type A. What actually counts is your blood level of vitamin C.
Animals keep their blood levels of vitamin C at a constant of around 60 to 70 µmol/l. If they are exposed to a virus, or to stress, both of which deplete vitamin C, they just make more and always enough for some to spill out from the bloodstream into the kidneys and consequently into urine.
Make Sure You Pee Vitamin C
Those who say that vitamin C, especially in higher amounts, is just making expensive urine are correct, but fail to release that this is exactly how all animals are designed – to always have enough, and never too much, by excreting a little in urine. That is also why vitamin C is never toxic. You just pee out more. If you take in much more than you can absorb, this also triggers looser bowels, so thats another ‘safety valve’ the body uses to make sure it gets what it needs and no more. That’s another way you know how much you need under viral attack – however much you can tolerate before excessively loose bowels.
What this also means is that you know instantly if a person is vitamin C depleted by a simple urine sensitive vitamin C dip stick called Vitacheck. If it changes colour from blue to yellow you know you have an optimal intake. If it doesn’t change colour then you know a person is deficient. While not as definitive as a serum or plasma vitamin C blood test, it can establish if a person is critically deficient, and therefore at high risk, or optimally sufficient.
With 44% of covid deaths in care homes, and more in older people, especially males, with conditions such as diabetes and hypertensionHypertension is more commonly known as high blood pressure…., from higher deprivation zones, it is highly likely that 80 per cent or more of deaths are related to risk factors that are associated with low serum vitamin C.
Two Simple Steps to Cut Your Covid Risk Substantially
Given that 97% of people who become infected have minor symptoms, and of those having severe symptoms, the vast majority fit into these high risk camps, it is highly likely that ensuring vitamin C intake is always at optimum, defined by a simple urine test, would substantially reduce the risk of that 3%.
In addition, having an optimal blood level of vitamin D, certainly above 75nmol/l and ideally above 100nmol/l, is already established to massively reduce risk of severe covid. Three studies, from Germany, Italy and Spain show that ensuring adequate vitamin D cuts risk of mortality to a tenth of that of those who are deficient.11 Also, a study ensuring vitamin D sufficiency by giving hospitalised covid patients a high dose supplement of 532mcg(>10,000iu) of vitamin D reduced those admitted to ICU to 2%, with no-one given vitamin D dying, compared to non-supplemented patients, half of which ended up in ICU with two dying.12
Thus, these two simple actions – getting you blood level of vitamin C up to 100nmol/l, and ensuring you have vitamin C in your urine – could be a game changer for severe covid risk.
Most experts agree that taking in 1 gram of vitamin C twice a day when not infected is sufficient. Linus Pauling took 8 grams a day in his 80’s. Public health Professor Harri Hemila from the University of Helsinki says there is a case for taking 6 to 8 grams a day if at high risk of viral exposure. As a rule of thumb guideline you could add 1 gram for every risk factor – over 65, male, black, diabetic, hypertensive, COPD, blood type A, higher material deprivation. If all applied you could end up taking 8 grams a day. However, the beautiful thing is your body will tell you, either by hitting your bowel tolerance level or by hitting the yellow scale on the Vitacheck urine test.
As for vitamin D, while I generally recommend everyone supplement 15mcg (800iu) on a daily basis all year round, and get outdoors for 30 minutes every day as well as eating fish and eggs, this alone is not enough in the winter months if you live far north or south (basically above 40 degrees N or S latitude – the UK is above 50 degrees North). In that case I’d recommend a total of 2,000iu a day. If you are taking a multivitamin providing 800iu, this means ‘topping up’ in winter with an additional 9,000iu once a week, or three 3,000iu capsules once a week. There is no need to take vitamin D daily as it stores. A proportionate higher dose once a week is just as effective and less hassle.
These two acts could easily substantially reduce your risk of ever contracting severe covid.
DEATHS & ADMISSIONS GOING DOWN
There is good news: the number of deaths reported in those testing COVID-19 positive has gone down for the third week in a row. Both deaths and admissions into ICUs has gone down too.
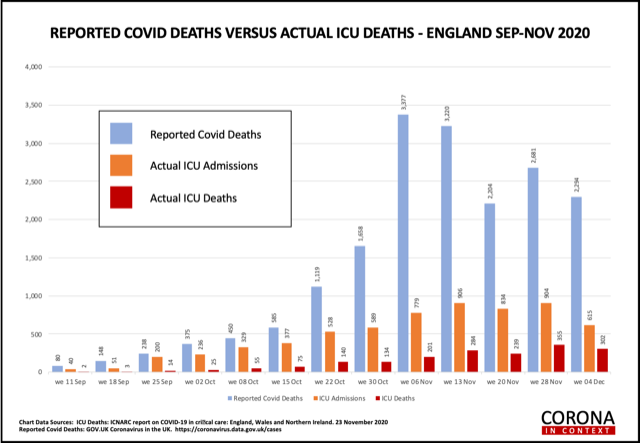
Deaths last week across all ICUs were 302 accounting for one out of 8 deaths recorded in those testing COVID-19 positive. Overall mortality for those admitted into ICUs stands at 29%. In other words more than 2 in 3 survive. This is a considerable improvement from the first wave average of 42% mortality. This no doubt reflects a learning curve in treating the ‘cytokine storm’ phase of this disease, however this would be expected to be much lower with the use of intravenous vitamin C. Now that the Chelsea & Westminster Hospital, who have started to test some of their ICU patients for vitamin C, have increased the dose given from up to 2g a day to up to 6g a day (listen to last week’s podcast on this) it is vital to see how this increased use of vitamin C plays out in their mortality rate which was 29% in the first wave.
BREAKTHROUGH IN EARLY PREVENTION OF COVID-19
Last Friday, in a press conference in the US, leading emergency medicine experts who formed the Frontline COVID Critical Care Expert Group (FLCCC) with the lowest mortality rate, below 5% with the ‘MATH+ protocol (including steroids (methylprednisolone), ascorbic acid, anti-coagulant heparin + other nutrients such as vitamin D and zincWhat it does: Component of over 200 enzymes in the body, essential for growth, important for healing, controls hormones, aids ability to cope with stress…) have shown how to massively reduce the spread of COVID-19 and how to treat COVID-19 at home to shorten infection and to prevent the development.
When a person is in a high risk community, for example a family member gets COVID-19 the odds of another family member getting COVID-19. There are four actions that work in such a situation – masks, social distancing, vitamin C and the anti-parasitical drug Ivermectin. This is a very safe and inexpensive drug based on over 3.7 billion doses showing remarkable safety. Like vitamin C, Ivermectin is helpful in both prevention in a high risk groups and in early treatment of infection.
Both vitamin C and Ivermectin massively reduce the risk of getting COVID-19 if exposed and the severity and duration of infection if given early. We also know that vitamin D and zinc play a crucial role. The purpose of this press conference, which you can listen to here , is to really show the world that we have an effective way to a) stop spread of infection; b) shorten duration and severity of infection and thereby prevent tipping into the acute inflammatory stage; c) cut mortality to below 5% in those critically ill COVID-19 patients, effectively saving all lives except for those over 85 and with an end stage disease.
REFERENCES
1. Patterson G, Isales CM, Fulzele S. Low level of Vitamin C and dysregulation of Vitamin C transporter might be involved in the severity of COVID-19 Infection, Aging and Disease 2021 Apr:12(2)
2. Arvinte C, Singh M, and Marik PE, Serum levels of VitaminC and Vitamin D in a cohort of critically ill COVID-19 patients of a North AmericanCommunity Hospital Intensive Care Unit in May 2020. A Pilot Study, Medicine in Drug Discovery (2020), DOI:10.1016/j.medidd.2020.100064
3. Fletcher AE, Breeze E, Shetty PS (2003). Antioxidant vitamins and mortality in older persons: findings from the nutrition add-on study to the Medical Research Council Trial of Assessment and Management of Older People in the Community. The Amer J Clinical Nut, 78:999-1010.
4. Mosdøl A, Erens B, Brunner EJ. Estimated prevalence and predictors of vitamin C deficiency within UK’s low-income population. J Public Health (Oxf). 2008 Dec;30(4):456-60. doi: 10.1093/pubmed/fdn076. Epub 2008 Sep 23. PMID: 18812436
5. Göker H, Aladağ Karakulak E, Demiroğlu H, Ayaz Ceylan ÇM, Büyükaşik Y, Inkaya AÇ, Aksu S, Sayinalp N, Haznedaroğlu IC, Uzun Ö, Akova M, Özcebe OI, Ünal S. The effects of blood group types on the risk of COVID-19 infection and its clinical outcome. Turk J Med Sci. 2020 Jun 4;50(4):679–83. doi: 10.3906/sag-2005-395. Epub ahead of print. PMID: 32496734; PMCID: PMC7379446.
6. Latz CA, DeCarlo C, Boitano L, Png CYM, Patell R, Conrad MF, Eagleton M, Dua A. Blood type and outcomes in patients with COVID-19. Ann Hematol. 2020 Sep;99(9):2113-2118. doi: 10.1007/s00277-020-04169-1. Epub 2020 Jul 12. PMID: 32656591; PMCID: PMC7354354.
7. Zietz M, Tatonetti NP. Testing the association between blood type and COVID-19 infection, intubation, and death. medRxiv [Preprint]. 2020 Apr 11:2020.04.08.20058073. doi: 10.1101/2020.04.08.20058073. PMID: 32511586; PMCID: PMC7276013.
8. See https://science.sciencemag.org/content/370/6515/eabd4585
9. Colunga Biancatelli RM, Berrill M, Marik PE. The antiviral propertiesof vitamin C. Expert Rev Anti Infect Ther. 2020;18:99–101. DOI: 10.1080/14787210.2020.1706483
10. Kim Y, Kim H, Bae S, Choi J, Lim SY, Lee N, Kong JM, Hwang YI, Kang JS, Lee WJ. Vitamin C Is an Essential Factor on the Anti-viral Immune Responses through the Production of Interferon-α/β at the Initial Stage of Influenza A Virus (H3N2) Infection. Immune Netw. 2013 Apr;13(2):70-4. DOI: 10.4110/in.2013.13.2.70
11. Radujkovic A et al, ‘Vitamin D Deficiency and Outcome of COVID-19 Patients’. Nutrients. 2020 Sep 10;12(9):2757. doi: 10.3390/nu12092757. PMID: 32927735; PMCID: PMC7551780. Carpagnano, G et al. Vitamin D deficiency as a predictor of poor prognosis in patients with acute respiratory failure due to COVID-19. J Endocrinol Invest (2020). https://doi.org/10.1007/s40618-020-01370-x;for Spanish Castillo study see below
12. Castillo ME et al., “Effect of Calcifediol Treatment and bestAvailable Therapy versus best Available Therapy on Intensive Care Unit Admission and Mortality Among Patients Hospitalized for COVID-19: A Pilot Randomized Clinical study¨ ,Journal of Steroid Biochemistry and Molecular Biology (2020), doi: https://doi.org/10.1016/j.jsbmb.2020.105751
Comments
Join the Conversation on our Facebook Page