The undeniable data I have access to every week is what’s happening in Intensive Care Units, supplied by the ICNARC (Intensive Care National Audit Research Centre) and the government’s reported number of tests, positive cases and ‘covid’ deaths (being anyone dying with a positive covid test in the last 28 days). What I can’t get is the ‘bit in the middle’, that is the weekly covid-related hospitalisations. No employee of the NHS is allowed to share this. I don’t know why this isn’t being made available. If it is somewhere please let me know.
Part of this disparity may be regional. For example, London has had half the ICU admissions and deaths of the NorthWest both in the last two weeks and since 1st September and the South West (inc Cornwall) has a quarter of those of London. The SouthWest, in the last fortnight, have had 73 people in a critical condition admitted in ICU. The NorthWest have had 288 admissions.
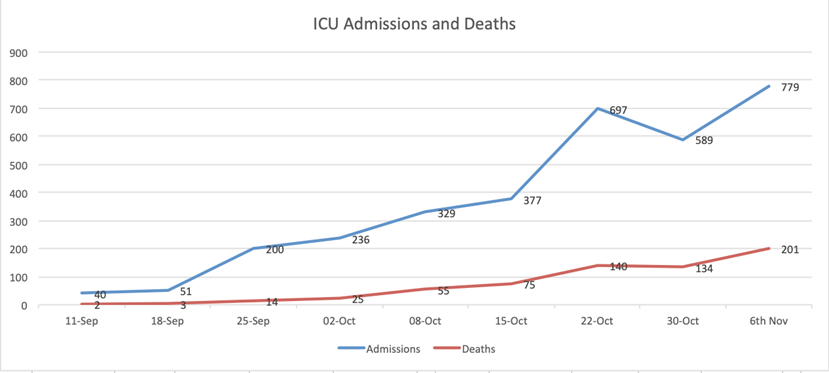
Last week, across all ICUs there were 201 deaths. As you can see from the graph below there is a slow but steady increase in ICU admissions and deaths roughly increasing by a third each week.
Are ICUs at capacity?
According to the Kings Fund NHS adult ICU capacity for covid is 4,100 beds. There are currently 1,200 in ICUs so that suggests the NHS ICUs are at about a quarter of national capacity. To cross check this divide 4,100 by the 286 ICUs and it suggests the average number of beds per ICU is 14. This may not be exactly right but is in the right ballpark. Neither the NHS nor ICNARC appear to publish their capacity which would be good to know.
You might think, oh my God, if numbers of admissions quadruple, which they could, ICUs will be swamped. That’s not quite true because the average length of stay in 5 days (survivors) and 8 days (non survivors) so people are leaving quite quickly. It’s probably got to go up more like eight fold to reach total capacity, but that’s also a bit misleading because some areas, like the NorthWest, especially if they have less ICUs for their population, may be reaching capacity, while others, such as Cornwall, may be empty. Even at the height of the first wave 28 ICUs had no covid patients and remained empty.
Who, where and why are people dying?
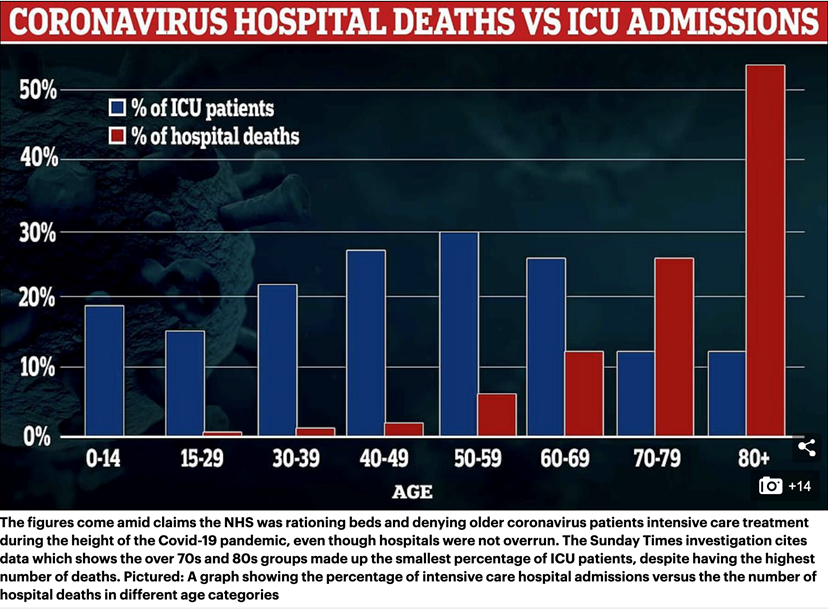
If you believe the ‘covid deaths’ are actually covid deaths then one in eight are dying in ICUs. So where are the remaining seven dying? There’s also a tiny percentage (3%) who leave ICU then die in hospital. This accounts for 40 further deaths in addition to the 649 people who have died in ICUs since September 1st. That makes 679 deaths in 8 weeks or 85 a week as an average so far. According to an article in the Daily Mail this big disparity between ICU deaths and so-called covid deaths is largely due to the non admission of older people, over 70, into ICUs. I suspect this is broadly true – that perhaps 4 or 5 of those 8 deaths are in older people, maybe in care homes or hospitals, but not admitted into ICUs. I suspect at least 2 or 3 so-called ‘covid’ deaths are not covid at all, but other events such as heart attacks or strokes.
But what exactly is it about being older that makes you unable to survive any flu or stop a harmless cold turning into a fatal respiratory infection? No doubt you’d say that they have less ‘resilience’. But what does that mean? An ICU in Colorado that has measured vitamin CWhat it does: Strengthens immune system – fights infections. Makes collagen, keeping bones, skin and joints firm and strong. Antioxidant, detoxifying pollutants and protecting against… levels of its patients, found that those who didn’t survive have much lower blood levels, often below the ‘scurvy’ level of overt deficiency, than survivors. But what intrigued me was that, while increasing age is an accepted predictor of likely mortality, when they factored in their vitamin C level age was no longer a predictor of mortality. But vitamin C level was. In other words, what we call ‘resilience’ may be in part a function of your reserves of vitamin C. The older you are the more you need to take in to maintain sufficient reserves to fight a cold. This means that eating an orange a day is nowhere near enough for an 80 year old. They have to supplement. Linus Pauling was supplementing 6 grams a day in his eighties. That’s why I think all older people in care homes should have a simple urine test for overt vitamin C deficiency and supplement accordingly. Also, they should be given extra vitamin DWhat it does: Helps maintain strong and healthy bones by retaining calcium. Deficiency Signs: Joint pain or stiffness, backache, tooth decay, muscle cramps, hair loss…. to boost blood levels to 100nmol/l.
I don’t think it is morally right to let our loved ones die of or with scurvy levels of vitamin C. It reminds me of my wife’s uncle David. He had untreatable cancer and was given two weeks max to live. So he was dispatched from hospital into a hospice. As often happens as someone approaches death all his medication was stopped. He also asked his daughter to go into his kitchen and get the box marked ‘Patrick’s vitamins’. Despite his death sentence he started taking his vitamins again. Whether it was that, or not being on medication, he soon perked up, left the hospice and went home to live for a further six months giving him time to get his affairs in order and bid farewell to his family. We ‘faked’ a Christmas and got the family together, knowing he wouldn’t make it.
All this talk of deaths can get you scared but 201 deaths this week in ICUs is very small compared to the usual annual 10,000 deaths a week, roughly 1,000 of which would be from flu and other respiratory infections, which have mysteriously fallen away. Unless I’m missing something major I can’t see the logic behind a total lockdown except perhaps in areas that are overloaded to protect NHS capacity. Locking down the most vulnerable makes much more sense to me. When you think of these small numbers against the suicides, depression, destruction of businesses, jobs and ensuing poverty, it just doesn’t make sense to me.
I’m writing this in the airport, returning from Denmark. I’ll be going into two week’s quarantine but why? Wouldn’t it make more sense to PCR test me on arrival, or within 3 days, then quarantine me if I test positive? (I didn’t stroke any minks.) If I was a critical health workers that would be one more man down potentially unnecessarily.
Is covid being more effectively treated?
The percentage of deaths to admissions in ICU is still going up, currently at 26% last week, compared to the previous week’s 23%, still lower than the 40+% at the end of the first wave. Given the lag I’ll not be confident we know the true improvement in treatment until the weekly percentage of deaths to admissions levels off. I also hope more and more ICUs will add intravenous vitamin C. I’m led to believe there are now at least a dozen. One has started testing vitamin C and, as a consequence, upped the intravenous dose to 6 grams. The best ICU results reporting 5% mortality are using 12 grams, giving 3 grams every 6 hours.
What’s your risk?
The good news, from last week is that, nationally, the rate of positive PCRs tests has gone down. This last week there were an estimated 507 positive tests per 10,000 compared to the week before, which was 758. That means 5 in every 100 people tested are covid positive. About 1% of those testing positive die.
Of course, this level of risk would no doubt be massively reduced if you are taking steps to boost your own immune system with a healthy diet including lots of berries, keeping fit and supplementing vitamin C, D, zincWhat it does: Component of over 200 enzymes in the body, essential for growth, important for healing, controls hormones, aids ability to cope with stress…, magnesiumWhat it does: Strengthens bones and teeth, promotes healthy muscles by helping them to relax, also important for PMS, important for heart muscles and nervous… and other antioxidants.
Stay well. Stay free. Patrick
For more information on how to protect yourself read Flu Fighters.
Comments
Join the Conversation on our Facebook Page