
Last month I did a post headed ‘Don’t Jump the Gun on the Pfizer Vaccine’ saying we should wait until, at least, there is a published study in a peer-reviewed journal.
The Pfizer vaccine results have been published this month in the New England Journal of Medicine. They demonstrate a 50% efficacy after the first vaccine dose and a 94-95% efficacy after the second vaccine dose. Efficacy here means identifying the number of symptomatic COVID cases in the vaccinated group versus the unvaccinated group.
This is calculated from dividing the number of covid cases in the placebo group, namely 162 out of 18,325 (9%) vs 8 covid cases in the vaccinated group of 18,198 people (0.04%) which gives 95% efficacy. This is not quite as impressive as it sounds. The one thing not reported is any COVID deaths in either group. This I find strange but remember the numbers of symptomatic cases are small (170 people). As the vaccine is rolled out this will be a vital outcome since saving lives is a major part of the reason for doing this. Given that over 18,000 people were vaccinated in relatively high
risk areas that’s a lot of people to treat for no covid deaths prevented.
There does not seem to be much variation in efficacy across age groups over age 16 (no-one under 16 was included in this trial), sex or race, which is good news as most vaccines are less effective in older age groups. The incidence of serious adverse events was similar in the vaccine and placebo groups (0.6% and 0.5%, respectively). Since the vaccine has been rolled out there have been eight cases of anaphylactic shock, possibly relating to the PEG (polyethylene glycol) component of the vaccine. No case was recorded in the trial.
The incidence of adverse events was 27% versus 12% in the placebo group or, when investigated to see if likely to be related to the vaccine, 21% versus 5%. Most appear to be transient. Severe fatigue was observed in approximately 4% of vaccine recipients, which the authors state is higher than that observed in recipients of some vaccines recommended for older adults.
What does all this mean? According to Zoe Harcombe “If you stopped 100 intelligent people in the street and asked them what 90% vaccine efficacy means, they will likely say that it means 90% of people vaccinated won’t get the virus. The fact is that 99% of people who were given the placebo didn’t get the virus. The intelligent person in the street won’t realise that it means approximately 100 people need to be vaccinated to avoid 1 case. They might think those vaccinated won’t have a bad outcome and can no longer transmit the virus. They probably won’t realise that the trials were not even designed to test these key issues. On the one hand, getting to vaccine approval in the same number of months that normally takes years is an extraordinary feat. On the other hand, the gap between what these vaccines can do and what people think and hope they can do is tragically wide.”
how do mRNA vaccines work?
The Pfizer and Moderna mRNA vaccine is a new technology. It works like this. When a virus gets into a cell of a muscle it puts some of its genetic material (RNA) into the DNA of the cell it has invaded. This mRNA contains instructions to make part of the virus’s ‘coat’- the distinctive spike proteins that stud its surface.
Ideally, from our point of view, the fragments of the viral coat, are spotted by the immune system which then mounts an attack and will recognise that particular proteinProteins are large molecules consisting of chains of amino acids. Proteins are essential nutrients for the human body – they are a building block of… in the future. Then according to Pfizer’s PR material, the inserted instruction is destroyed. But because of the lack of transparency, we don’t know whether it works like that or what side-effects it causes.
We do know that, unlike other vaccines, this mRNA vaccine doesn’t need an ‘adjuvant’ – the compound such as aluminium or mercury – that’s needed to trigger an immune response. Instead it contains a detergent known as PEG (polyethylene glycol) presumably to help insert the RNA into your cell’s DNA. So far two people in the UK who received the vaccine in a trial are known to suffered anaphylactic shock, a potentially fatal allergic reaction that can stop you breathing. The packet warns you shouldn’t take this vaccine if you have a history of allergic reactions. However, according to the New York Times, there have two more anaphylactic reactions in people in Alaska, one of whom had no history of allergy.
What does the Oxford vaccine trial show us?
The Oxford/AstraZeneca vaccine, the only one to publish its results in a peer-reviewed journal, is a chimpanzee adenovirus vaccine vector which contains the genetic sequence of the surface spike protein. When the vaccine enters cells in the body, it uses this genetic code to produce the surface spike of the coronavirus to induce an immune response The first adenovirus-based vaccine (a vaccine for Ebola) was approved for general use in July this year. The details of this vaccine are set out in a 14-page report in the Lancet. The report shows that the vaccine is 70% effective, meaning that out of 5,807 vaccinated volunteers 30 – or 0.5% – of them became infected or had at least one symptom.
That looks impressive and was a better result than the same sized control group who got a meningitis vaccine. More of them tested COVID positive – 1.7% vs. 0.5% = 70% – and two were badly infected, one of whom died. Another way of putting this is that vaccinating 5,000 people may have saved one life over the period of the trial. It’s hard to do statistics on 1 vz 0, which is why the meaningful effect on mortality is going to take longer to discover. If, however, valid that’s what we call an NNT (numbers needed to be treated for benefit) of 5,000.
Vaccines are always less effective in older people, whose immune systems tend to be less effective, but as yet we don’t have enough data to say how many it might protect – around 50% of those over 65 is a reasonable estimate. The Oxford group will publish results for this age group but they need enough people to become infected.
Can you test for immunity?
There are two ways to become immune – either by surviving an infection or by getting vaccinated – but as yet there is no reliable test to tell whether you are. The standard test for immunity, known as IgG, is to check for the antibodies in the blood that are produced by an infection. But that hasn’t proved definitive. Some who were infected don’t have them. Another test checks for something called T-cell memory. T-cells are part of immune system cells that remember previous infections. But people who have clearly been infected can show up as antibodyAn antibody is a protein produced by the body’s immune system when it detects a harmful substance known as an antigen. Examples of antigens include… negative and T-cell memory positive. The trouble is that T cell memory tests aren’t yet commercially available. So we still can’t check for ‘herd immunity’ – how many people in the population are protected.
Given this uncertainty I’d say that if you do have antibodies or T cell memory there’s not much point being vaccinated. If travel is restricted, it should only apply to people who haven’t been vaccinated or haven’t been tested for protective immunity, be it with antibodies or T cell memory.
Vaccine Adverse Effects – The Story So Far
What about adverse effects? We don’t yet have enough information about the Oxford vaccine – the only one I can comment on as it is the only one with published results – to know in detail how many may be damaged by it. The number of serious adverse reactions among those getting the Oxford vaccine and those in the meningitis group was about the same – 79 in the covid vaccine and 89 in the meningitis vaccine group. That suggests that for every 100 people vaccinated you can expect one or two to have a serious adverse reaction.
One worrying sign was two cases of something called ‘transverse myelitis’ which means a degeneration of the myelin sheath around nerves, as seen in multiple sclerosis. One was in the covid vaccine group and one in the ‘control’ meningitis group. There was a third case but it’s not yet known if they were given the covid or meningitis vaccine since they are in part of the trial that hasn’t been ‘unblinded’. It’s not clear why this would happen but it’s not an unknown adverse effect of vaccines. The Oxford paper doesn’t give details on other types of adverse reactions. It says that ‘all trial participants have recovered, or are in a stable or improving condition.’
Since the Pfizer vaccine has been rolled out there have been eight cases of anaphylactic shock, possibly relating to the PEG (polyethylene glycol) component of the vaccine. No case was recorded in the trial.The incidence of adverse events reported in the paper was 27% versus 12% in the placebo group or, when investigated to see if likely to be related to the vaccine, 21% versus 5%. Most appear to be transient. Severe fatigue was observed in approximately 4% of vaccine recipients, which the authors state is higher than that observed in recipients of some vaccines recommended for older adults.
However, since then, a CDC report has documented approximately 2%, or 1 in 50, have a ‘Health Impact Event’ which is defined as ‘unable to perform normal daily activities, unable to work, required care from doctor or health care professional’.
The reality is that we won’t know the full story on adverse effects for several months as we move into the surveillance phase and doctors make reports of adverse effects. There is no guarantee, at this point, of safety. Why some react and others don’t is also yet to be determined. In the end it will be about the numbers – how many have a disabling reaction which may or may not resolve versus how many covid deaths are avoided?
Prevention – an Alternative Approach – IVERMECTIN
So far, we have all been told that our only hope of beating the virus is with a vaccine which comes with inevitable risks and a very heavy price tag. But what if there was another strategy that looked promising, had virtually no side effects and would cost a tiny fraction of the budget for the vaccine? One that could easily be combined with rolling out the vaccine, which it might even make more effective.
The idea is to cut the risk of you getting infected and then if you do, to provide an effective treatment. It involves the familiar infection fighters vitamins C and D, along with a newcomer that few readers will have heard of – Ivermectin.
This is an old, off-patent drug, known to be very safe that has been used for nearly 40 years to treat parasitic infections. But there is also research showing it can block and kill a range of viruses including Covid-19. It also damps down the deadly inflammation that can develop with Covid and makes it less likely that infected people will pass on the virus.
If that all sounds dangerously too-good-to-be-true, there is a detailed report available on-line at (https://covid19criticalcare.com/wp-content/uploads/2020/10/FLCCC-IVERMECTIN-Summary.pdf) compiled by the Critical Care and Emergency Medicine group in the US. This is made up of critical care specialist who use a combination of nutritional supplements and drugs and whose units have been reporting remarkably low hospital mortality rates of between 4% and 10%.
This is what the new approach involves:
PREVENT INFECTION
- Supplement 1g of vitamin CWhat it does: Strengthens immune system – fights infections. Makes collagen, keeping bones, skin and joints firm and strong. Antioxidant, detoxifying pollutants and protecting against… twice a day.
- Supplement 1,000iu of vitamin DWhat it does: Helps maintain strong and healthy bones by retaining calcium. Deficiency Signs: Joint pain or stiffness, backache, tooth decay, muscle cramps, hair loss…. daily, or whatever you need to get your blood level above 75nmol/l.
- Take 1 Ivermectin pill a month, especially for those in high-risk areas. This totally safe drug, like vitamin C, effectively stops viral replication.
At the very least, this is likely to cut you risk of symptomatic infection by a factor of ten.
EARLY TREATMENT TO SHORTEN INFECTION
- Supplement 1g of vitamin C 8 to 20 times a day.
- Supplement 1,000iu of vitamin D daily, or whatever you need to get your blood level above 75nmol/l.
- Take 1 Ivermectin pill a month, especially for those in high-risk areas
- Supplement 60-100mg of zincWhat it does: Component of over 200 enzymes in the body, essential for growth, important for healing, controls hormones, aids ability to cope with stress… daily.
This protocol is likely to shorten an infection to under 48 hours, which means there won’t be enough viral load and dead virus particles left to trigger the acute inflammatory reaction that occurs in critical COVID-19. So it could totally eliminate COVID-19 deaths.
Are such results really plausible? Let’s take the vitamin D component. In the Spanish Castillo trial involving hospitalized COVID-19 patients who were already very sick, half were given a single very high strength dose of vitamin D. None died and and only 2% ended up in ICU. In the placebo group 50% went into ICU, where 15% died. If you look at Table 2 in our vitamin C review, you will see that mortality is reduced in almost every trial giving vitamin C versus placebo. So, the combination of vitamin C and D is highly likely to end, or massively reduce, ICU admissions.
EFFECTIVE TREATMENT OF CRITICAL COVID
We already know how to reduce mortality to under 5% in critical COVID-19 cases. It involves a protocol developed by the Critical Care and Emergency Medicine group called MATH+). This effectively eliminates deaths among those who do not have a pre-existing end-stage disease and are over 85.
MATH+ involves
- 12g of intravenous vitamin C (Chelsea & Westminster ICU in London is using up to 6g)
- Intravenous steroids such as methylprednisolone or dexamethasone
- Maximum dose anticoagulants such as Heparin
- Ivermectin
- High dose vitamin D
The NNTB (number needed to benefit) is 1. In other words, everyone benefits. So far there has not been a single serious adverse effect reported from units using these prevention and treatment approaches.
Vaccines or vitamin-based prevention?
These two approaches are not exclusive, and you can use the same mask, social distancing and lockdown strategies to reduce spread.
Currently the deaths among those who were positive on the COVID PCR test stands at about 1,500 a month (September to now). That translates to a projected 18,000 deaths in the year September 2020-21 assuming everything stays the same (in reality flu deaths go up until Feb, then vanish by April). So, let’s imagine you vaccinate, not 5,000 but 50 million (the UK adult population) and assume 70% efficacy.
If we save one life in 5,000 in the short-term, it’s reasonable to assume that in the longer-term double that will be saved. But the downside is that up to 10,000 are also likely to have a serious adverse reaction.
Alternatively, what happens if we follow the supplements plus drugs option? There is a good chance it will dramatically reduce the spread of infection and hospitalizations. And even if 1% of the 2 million expected to test positive over the next year end up in hospital (20,000) that will still produce a better result.
They would be given higher dose vitamin C and D, plus Ivermectin. At most, 2% could end up in ICU (400 people), where effective treatment would mean that only 5% (20) die. Result: 17,980 lives saved with no serious adverse reactions.
The benefits of the supplement plus strategy are considerable. It is easier, with the right promotion and education, it would meet less resistance from the public, the cost would be massively less and the strategy could be expected to work for future coronavirus mutations.
I want to emphasise that I am not anti-vaccination, even if I am hesitant about a vaccine until trial results are actually published. If I were in a vulnerable group, however, and wasn’t taking vitamin C, vitamin D or Ivermectin, and didn’t have a nearby hospital with an ICU which knew how to treat critical COVID-19 effectively, then, sure, I’d take the Oxford vaccine. I’m more hesitant about an mRNA vaccine both because nothing’s published, but also because it’s new technology involving inserting genetic code into my cells. I don’t yet understand how the code that makes me produce coronavirus spike proteins is then deleted.
I’m not going to because I am relatively young (62), have no risk factors and know how to prevent serious infection. You could say this is selfish – shouldn’t I take one for the team and help not infect others. But what I’m doing achieves the same end – not infecting others. I’m pleased that there are many people who would like to be vaccinated, although I seriously doubt they are being given full information required for informed consent.
That seems to me to be a fair appraisal of where the science is at now. The biggest failing by our governments and the health authorities is their continuing refusal to even consider the growing evidence for vitamin C, D and Ivermectin. I believe backing only vaccination it will come to be seen as a disastrous decision.
ICU DEATHS AND ADMISSIONS LAST WEEK are down BY A THIRD
Last week, up to Friday, both ICU admissions and deaths are down. The trend over the month is certainly downwards while one would normally expect, with winter flu, the opposite. See the graph below.
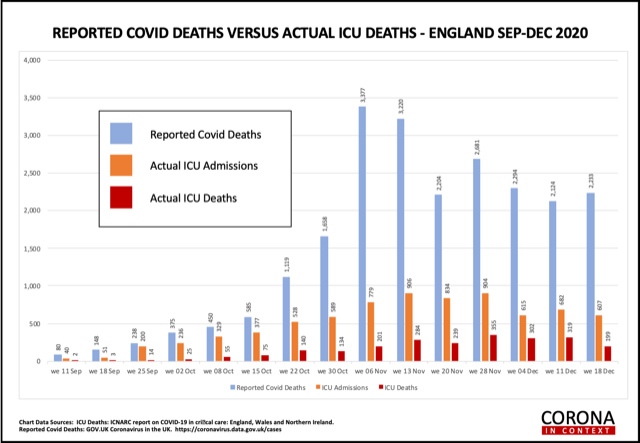
These are figures given to me every week from the Intensive Care National Audit Research Centre, who receive results from all UK ICUs. As such, they are a very reliable source of information. To put this in context your risk of dying in an ICU following testing COVID positive is 0.16% or 1 in 625.
A greater percentage of people tested last week are testing COVID-19 positive (5.7%) than the previous week (3.6%) but less than a month ago (6.8%). WHO guidelines support lockdown when the percentage is over 5%. Deaths of people testing COVID-19 positive are also up and less deaths last week (one in 11) occurred in ICUs compared to the previous three weeks where 1 in 8 died in ICUs. So, hospitals probably have more patients overall, but ICUs do not. Overall, ICUs have a lower mortality, of 31% (previous two weeks were 30%) possibly indicating that treatment is becoming more effective. It certainly seems to be levelling out at around 30%, compared to the first wave’s average of 42%.
DEATHS FROM NON-COVID CAUSES DECLINE AS COVID DEATHS INCREASE
Part of the reason for the increase in deaths of people testing positive for COVID-19 is reclassification. The analysis below of deaths in October, from the Office of National Statistics, show that all other top ten casuses of deaths, and especially flu/pneumonia, are considerably lower.
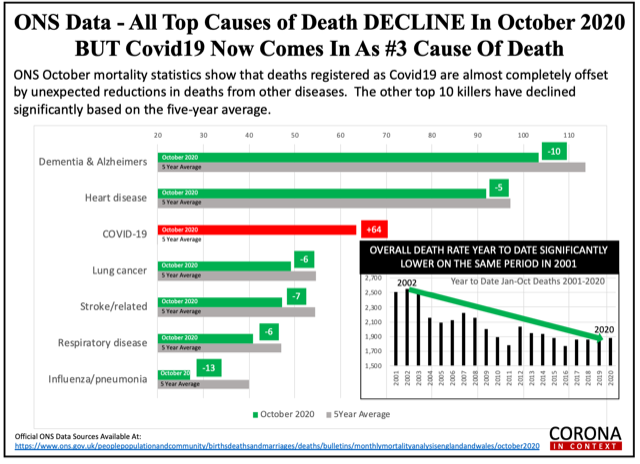
Since you cannot be classified both as a COVID positive death and a flu/pneumonia or dementia death, this skews COVID positive deaths to the third most common cause of death in October. I don’t see why it couldn’t be done the other way around. Eg if someone die of dementia, heart disease, lung cancer or stroke etc, but happens to have tested posotive yet has no symptoms as such of COVID-19 then they would be allocated to the disease rather than COVID. Why scare people unnecessarily? I can understand that respiratory/flu/pneumonia deaths might be a bit hard to separate since they have overlapping symptoms but, if you look at the chart below, and deducted these from the COVID positive deaths then COVID positive deaths would be ranked much lower.
Remember to take your vitamin C and D, as well as zinc, over Christmas and eat lots of cabbage and brussels sprouts, as well as satsumas – and wear your mask in public places.
Wishing you a Happy Christmas and Healthy New Year, Patrick
KEEP INFORMED
Sign up to my newsletter on the home page of this website to receive monthly COVID NEWS updates.
Comments
Join the Conversation on our Facebook Page