
COVID BOOSTERS – SHOULD YOU HAVE ONE?
If you’ve been vaccinated should you have the booster? With evidence published in the Lancet that “Pfizer vaccine effectiveness against all [covid] infections waned during the six-month study period, from 88% during the first month after receiving two vaccine doses to 47% after six months”, it seems that either vaccines don’t work so well against delta or the efficacy is waning. It’s probably a bit of both. Booster vaccines are the same – not strain specific or adapted for delta.
The case to have the booster is perhaps less compelling for someone who has had covid. According to Pfizer’s biochemist Nick Karl “When somebody is naturally immune … they probably have more antibodies against the virus. When you actually get the virus, you’re going to start producing antibodies against multiple pieces of the virus … So, your antibodies are probably better at that point than the vaccination.” A UK expert told me “We seem to see that with the more doses or, even better, a bit of vaccine and then a bit of natural infection, the strain breadth of protection increases. This is not what we expected.”
Although viral load after infection with the delta variant was shown to be similar in a vaccinated versus non-vaccinated person, it is possible that the vaccinated person may be less likely to become symptomatic, and even less hospitalised, based on pre-delta studies published in the British Medical Journal. While positive covid cases appear higher (per 100,000) in vaccinated than unvaccinated, emergency admission into hospital and deaths are substantially lower in vaccinated than unvaccinated, per 100,000. The actual numbers of vaccinated people, for example in my age group, presenting for emergency care were almost twice as high in September (402 in week 34 to 37 vs 790 for double vaccinated) but that is to be expected since the majority in my age group have been vaccinated.
Those against vaccines will say that more vaccinated people are becoming infected, and those pro vaccination will say the opposite claiming that it’s the unvaccinated that are filling hospitals, it’s important to look at the facts as known.
One example that was given to argue that ten times more vaccinated than unvaccinated were becoming symptomatic was an outbreak of SARS-CoV-2 Delta variant in an Israeli hospital where 42 patients, staff and family members became infected; 39 were fully vaccinated, reported in Euro Surveillance [P.Shitrit- Euro Surveill. 2021]
The infection or ‘attack rate’ as it is called was 10.6% (16/151) among exposed staff and reached 23.7% (23/97) among exposed patients in a highly vaccinated population, 16-26 weeks after vaccination (median: 25 weeks). All cases were linked and traced to one patient. Fourteen of 23 patients became severely sick or died, raising a question about possible waning immunity.
39 out of 238 vaccinated people were infected (16%)
3 out of 10 unvaccinated people were infected (30%)
On the face of it this did show that more ten times more vaccinated people (39 versus 3) became infected but given that more staff and patients were vaccinated than unvaccinated this is not so surprising. When you look at the percentage of vaccinated or unvaccinated who became infected the vaccinated were half as likely to become infected (16% versus 30%).
If over 80% of the UK population have been vaccinated, if vaccines were ineffective we’d still expect 80% of patients in ICUs to be vaccinated. If, for example, only half of those entering ICUs were unvaccinated then it would suggest that the vaccinated are less likely to become critically ill.
It is looking clear that vaccination does, and will continue to reduce hospitalization. I asked the Intensive Care National Audit and Research Centre (ICNARC) who collect data every week from all ICUs but don’t record vaccine status. They said a further study was underway.
What is also clear is that the effectiveness of vaccines fades quite fast. The latest study in the Lancet reports that the Pfizer vaccine effectiveness against infection waned progressively from 92% at day 15-30 from vaccination to 47% at day 121-180, and from day 211 (7 months) and onwards no effectiveness could be detected. In contrast, effectiveness of the AstraZeneca vaccine ‘was generally lower and waned faster, with no effectiveness detected from day 121 (4 months). Overall, vaccine effectiveness was lower and waned faster among men and older individuals. If you’re on the vaccine train you’re going to need boosters at least every six months.
DO BOOSTERS WORK?
Provisional results suggest they do but, as usual, Pfizer release results before peer-review and publication, so it’s their word. Also, the measure of success is not against a placebo but compared to those double vaccinated with Pfizer. So, if the first double jab’s immune protection wears off there’s more room for improvement. In the UK most had Astra Zeneca jabs first, and at a different interval, so results are not directly comparable.Also, any who had serious adverse effects are unlikely to sign up for such comparison trials.
ARE THE UNVACCINATED BEING ‘SELFISH’?
The moral ground taken by pro-vaccine people is that the unvaccinated are being selfish but there is a world of difference between an unvaccinated person who has a high vitamin DWhat it does: Helps maintain strong and healthy bones by retaining calcium. Deficiency Signs: Joint pain or stiffness, backache, tooth decay, muscle cramps, hair loss…. level, takes vitamin CWhat it does: Strengthens immune system – fights infections. Makes collagen, keeping bones, skin and joints firm and strong. Antioxidant, detoxifying pollutants and protecting against… for prevention (and Ivermectin if they could get it) and knows to take high doses upon infection, isolating and/or wearing a mask when out if symptomatic and someone who does none of these things.
Given that the viral load, upon infection, appears to be similar in a vaccinated and unvaccinated person the critical unknown is a) the difference between those who become symptomatic and b) the length of infection, which are the two critical factors that determine if an infected person will infect another.
Studies of asymptomatically versus symptomatically infected people’s ability to infect others shows that 4% of people become infected from a person with symptoms and 1% from an a symptomatically infected individual.
What’s more half of those who become infected from an asymptomatically infected person also become asymptomatic. So, if you become infected and remain asymptomatic you are not going to be a ‘super-spreader’.
One of the questions I’d like to know the answer for is how long a vaccinated but infected person remains infected so we could compare this to the known reduction in resolution of symptoms in someone taking vitamin C. With 8 grams a day given some days into infection this cuts the duration of infection by about 20%, improving recovery rate by 70%. I suspect, with 1 gram an hour or equivalent this could by reduced considerably but this has only been shown anecdotally.
Prior vitamin D status is also important in this regard, more than supplementation upon infection. Vitamin D deficiency increases risk for testing positive while having a high vitamin D level of 125nmol/l appears to reduce risk of infection by 50%.
VACCINE ADVERSE EFFECTS
Aside from sudden death, examples of side effects from vaccines include persistent malaise and extreme exhaustion, severe allergic, including anaphylactic reactions, multisystem inflammatory syndrome, psychological disturbances, seizures, convulsions and paralysis, including Bell’s Palsy. MHRA has just added another rare side-effect, Guilleme Barre syndrome, to AZ’s vaccine black box, joining thrombocytopenia. Overall, the adverse reaction rate is 1 in 150 although the true adverse reaction rate will be higher due to under-reporting.
Most reactions are minor and resolve but not all do. According to the UK Government, ‘From analysis of UK and international data, there has been a signal of an increase of cases of myocarditis and pericarditis following vaccination with both Pfizer/BioNTech and Moderna vaccines.’ This is a swelling and inflammation of the heart.
The biggest area of concern, especially with the mRNA vaccines, is a disturbance in blood clotting. Confusingly, when abnormal clotting occurs it uses up platelets which float around in the blood and are need for clotting, so then platelet count drops which can lead to haemorraging and bruising. Evidence of abnormal clotting is emerging both post-vaccine and post covid. For those whose symptoms do not quickly abate I recommend high dose vitamin C, up to bowel tolerance, as one would do for infection. For those more cautious, a few days of high dose vitamin C following vaccination is not a bad idea. Bromelain, a proteinProteins are large molecules consisting of chains of amino acids. Proteins are essential nutrients for the human body – they are a building block of… digesting enzyme, is helpful for breaking down clots. Together with quercetin, these three nutrients are proving effective in long covid. Karen is a case in point and you can view her experience here.
VACCINE ASSOCIATED DEATHS
In the UK gov.uk records 1,698 records of deaths shortly after vaccination considered by a doctor to be worthy of a yellow card report according to .gov.uk. This is a rate of 4 per 100,000 vaccinated.
This is slightly higher than the annual risk of dying in a traffic accident (1,472) and twice the risk of a woman dying from cervical cancer (850). These vaccine associated deaths are written off a line ‘Review of individual reports and patterns of reporting does not suggest the vaccines played a role in these deaths.’ This statement has remained the same throughout the pandemic with no link to any review.
A small number of these deaths have been due to thrombocytopenia, relating to the Astra Zeneca vaccine. Up to 6 October 2021, the UK’s ‘MHRA had received Yellow Card reports of 424 cases of major thromboembolic events (blood clots) with concurrent thrombocytopenia (low platelet counts) in the UK following vaccination with COVID-19 Vaccine AstraZeneca. Forty six of the 424 reports have been reported after a second dose. Of the 424 reports, 213 occurred in women, and 207 occurred in men aged from 18 to 93 years. The overall case fatality rate was 17% with 72 deaths, six of which occurred after the second dose.’
These numbers may be small given the millions of vaccination doses but they are still a cause for concern – and also likely to be under considerably reported by a factor or two to ten, as has been shown for other treatment-related reports of deaths using the yellow-card reporting scheme.
The risk/benefit equation certainly doesn’t stack up for vaccinating children or healthy people under 60 who know about prevention with vitamin C and D.
FOLLOW THE MONEY
The pattern of ignoring adverse effects, overplaying benefits, killing off competitors and generating a climate of fear where sales can flow is a standard marketing story for new drug pushes. We should expect this and be primed for it hence suspicious rather than surprised. Pfizer and AstraZeneca have been collectively fined over $3.6 billion for off-label promotion, fraud or kickbacks where prescribers get paid.
Airfinity put total market sales for COVID vaccines in 2022 at $124 billion, according to the Financial Times. Pfizer vaccine sales are predicted to reach $54.5 billion in 2022, and Moderna’s will hit $38.7 billion. The estimates blow the earlier figures — $23.6 billion for Pfizer and $20 billion for Moderna — out of the water.“The numbers are unprecedented,” Rasmus Beck Hansen, CEO of Airfinity, told the Financial Times. Sales of the mRNA shots will continue to rise in 2022 due to boosters and countries stockpiling to ward off variants, Airfinity said. Pfizer will generate 64% of its sales, and Moderna 75% of its sales, from high-income countries in 2022, the analysts predicted.
FLU JAB – YES OR NO?
Are you going to have the flu jab this winter? Firstly, let me make it clear that there is nothing new or different about this year’s flu vaccine compared to last other than the blend of viral strains in the mix. It does not contain a coronavirus component.
Last year’s flu jab was 29% effective, ranging from 37% effective in the age group of 2-17 and 26% in the over 65’s. This means that three in ten having a shot, if exposed to flu, may not to succumb or will recover more speedily. But these observational studies, quoting an article in the British Medical Journal headed ‘Doubletalk hides serious problems with flu shot safety and effectiveness’ says “They do not mention that these studies make no effort to look for adverse vaccine effects (e.g. narcolepsy, seizures, high fever, oculorespiratory syndrome). They do not mention “negative vaccine effectiveness”, the increase in risk of illness from influenza and non-influenza viruses associated with (or caused by) the vaccines. They do not mention that a vaccine “effective” in one season may increase influenza risk in a subsequent season. (Read about “antibody-dependent enhancement” to understand one explanatory mechanism). They do not mention that the observational studies they refer to are likely to exaggerate vaccine effectiveness in the first place because of the “healthy user effect” well known to epidemiologists.”
Personally, at the age of 63, I’m not going to have the flu vaccine but I entirely respect someone who chooses to, perhaps because they are older, more vulnerable, with more compromised immune systems.
These are my reasons:
1. The flu jab, for my age group, is unlikely to be more than 30% effective. So, what should one do for the 2 in 3 flus that vaccination won’t help?
2. A comprehensive review of vitamin C shows up to 46% reduction in duration of colds, and also reduction in severity, reported in those taking 8 grams of vitamin C in the first day of a cold/flu, although there is some evidence than 15-20 grams within 24 hours of first symptoms would be more effective. This is what I do, and recommend, taking around 1 gram an hour, or 2 grams every two hours. If your vitamin C also has zincWhat it does: Component of over 200 enzymes in the body, essential for growth, important for healing, controls hormones, aids ability to cope with stress… and black elderberry it is likely to be even more effective. I very much doubt flu would ever be fatal if all ‘at risk’ eg elderly people did this on first signs of symptoms.
3. I take 3,000iu of vitamin D3 to get my vitamin D level up to 120nmol/l. At this level the risk of dying from flu, or covid, is effectively zero anyway, according to David Grimes (hear his podcast interview on patrickholford.podbean).
4. There is a risk of adverse effects. Also evidence that those vaccinated are more susceptible the following year. I’m concerned about the effects on children and pregnant mothers. Again, quoting the BMJ ‘large cohort study found that flu shots given during the first trimester of pregnancy were associated with a 20% increase in autism spectrum disorder in the offspring’.
The authors acknowledged that, if it was causal, it would mean four additional autism cases for every 1000 mothers vaccinated.’ In the UK it’s virtually impossible to get any reliable data on numbers. While I’ve read reports of deaths associated with last year’s flu vaccine, I also know that the UK government is in so much denial that any vaccines can harm anyone that I doubt we’ll ever have clear information on the scale of risk, which I assume to be small, but maybe greater in exactly those most vulnerable, with weaker immune systems, who thus are more likely to opt for the vaccine.
5. I don’t like putting aluminium, in any quantity, into my body. The flu jab contains aluminium as an adjuvant to spur the immune system to attack the viruses. Personally, I don’t want to inject aluminium, even in tiny quantities, into my body unless there’s a really compelling reason and no safer alternative.
6. The flu vaccine won’t create herd immunity. The ‘herd immunity’ argument – that if everyone is vaccinated the disease (for example, smallpox) can be eradicated – does not apply to the flu vaccine because the influenza virus is endlessly mutating into different forms. One could argue that, if all were vaccinated flu might spread less, but this would need to be demonstrated. Flu mysteriously vanished last winter. Was this a consequence of lockdown? Or were some flu deaths reclassified as covid deaths? This needs investigating. What happens this year will be telling.
7. The flu vaccine is unlikely to take the load off the NHS re covid-19. Firstly, it takes doctors and nurses to deliver vaccines so their time gets used up. Secondly, covid-related ICU admissions and deaths are not rising. Since the flu vaccine has no coronavirus component, just like last year’s, any dreams that it will reduce a person’s chances of getting covid-19 are not based in fact. If the goal was to take the burden off the NHS then getting everyone’s vitamin D levels up, and recommending daily vitamin C supplementation, and high dose vitamin C supplementation when infected would be easier and cheaper and, I’m proposing, more effective.
THIRD WAVE NEWS
Those following my COVID NEWS report know that I’ve been monitoring weekly COVID deaths within 28 days, plus deaths and admissions into ICU, as well as the percentage of people testing positive e.g. positive cases divided by tests. It has always amazed me that percentage of tests being positive is not reported by either the media or the government websites. Instead they report the number testing positive, which of course goes up if you test more people. As one professor of statistics said “if you test more people’s IQ you’ll find more morons.” It is such an easy and obvious add-on. WHO use above 5% of tests positive as a criterion for action. Currently were at 3.2%, having dropped from 4.4% wth covid deaths within 28 days of a positive PCR test down.
In the chart below you’ll see what’s happened for the past two months, up to now, as well as a comparison to the same time last year.
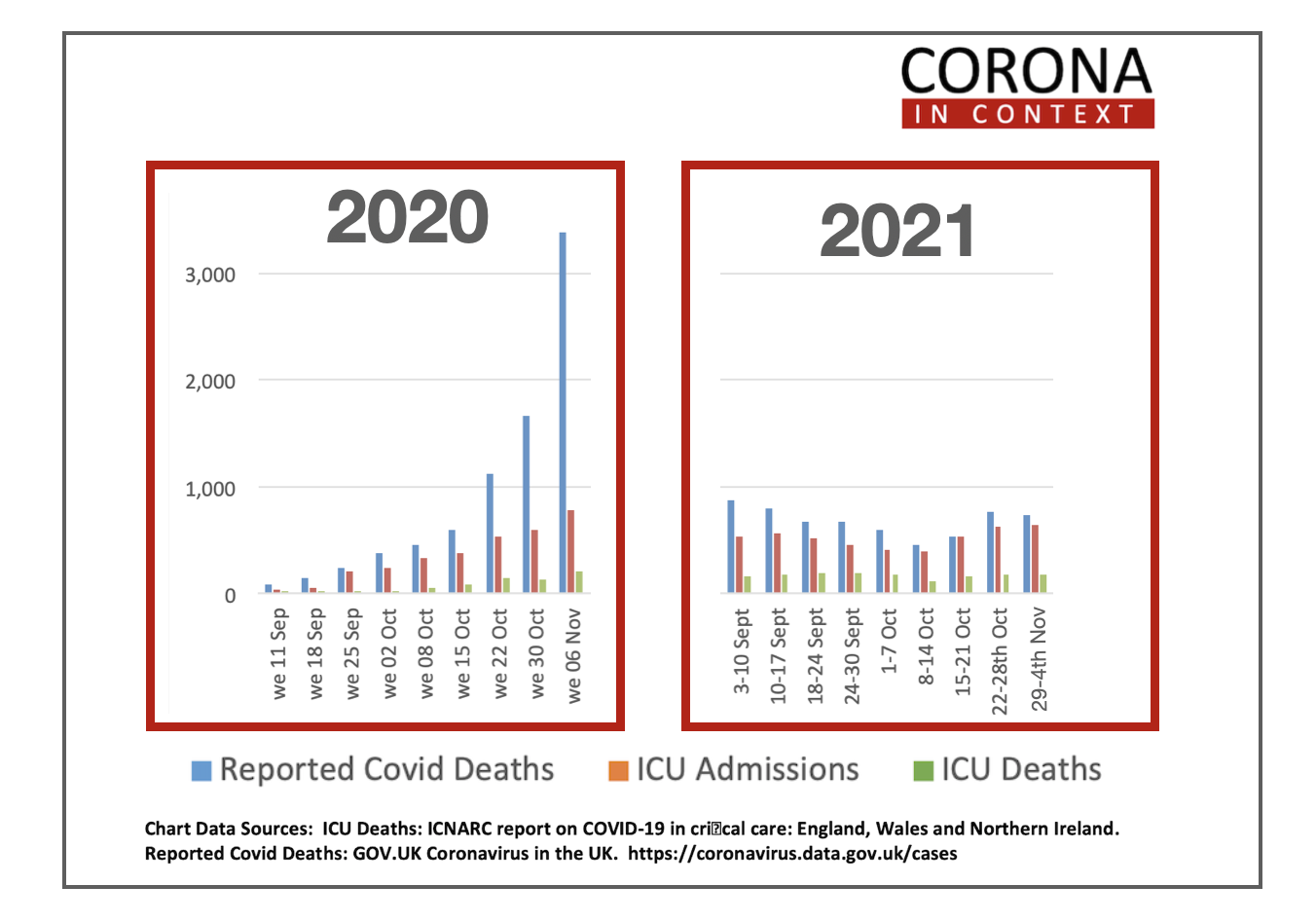
There’s no obvious trend in either deaths within 28 days of a positive PCR test, or ICU admissions or ICU deaths. Last year, these numbers grow week on week from the 1st September. This may be a consequence of a number of factors – delta variant being weaker, vaccination shortening infection, more people used to knowing what to do, more natural immunity are all possible contributors. Also, a greater percentage of covid deaths are happening in ICUs. It used to be one in eight and it’s now around one in four. So, if ICUs get better at treating, as they are, with mortality rate dropping from over 40% to well under 30%, then that’s good news. We do need them all to take IV vitamin C seriously.
Things may yet change but, right now, I don’t see any evidence of anything that could be called a third wave of covid deaths and hospital overloads this winter due to covid, although I suspect we’ll have a third wave of bullshit to drive the commercial agenda.
Comments
Join the Conversation on our Facebook Page