
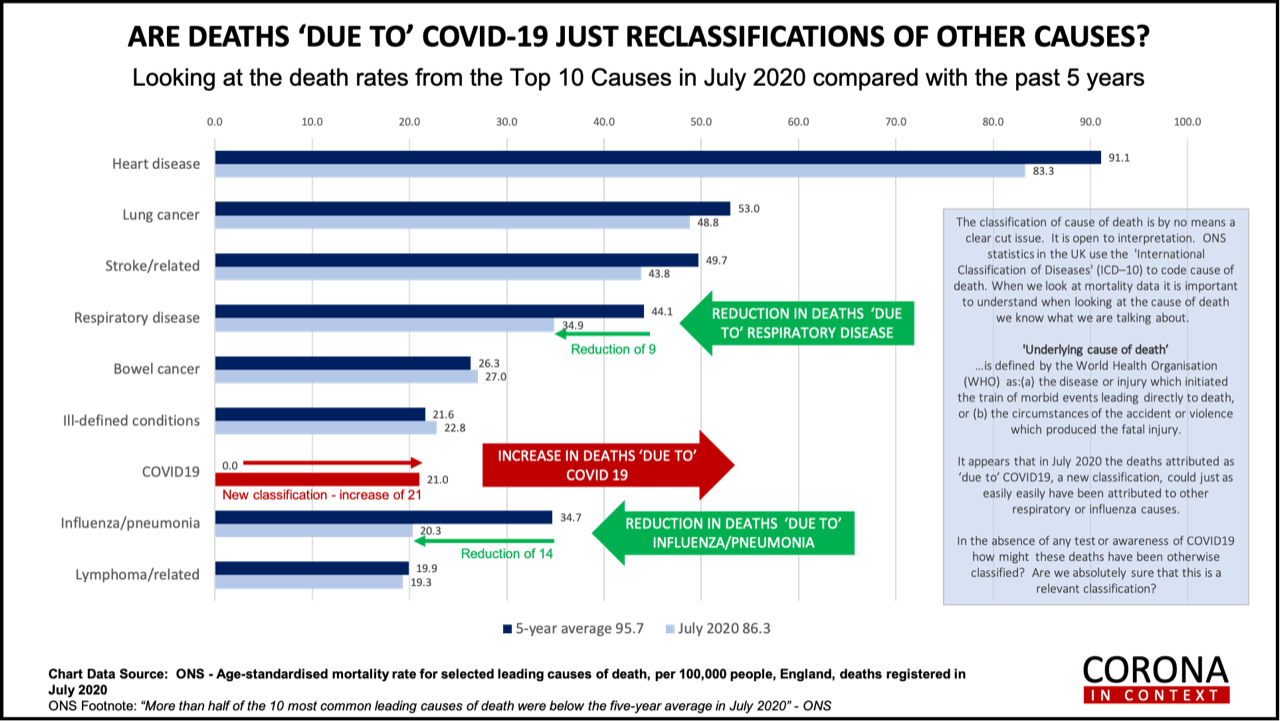
Cases are cranking up but what about deaths? I am distrustful of what recorded ‘deaths with covid’ actual means. Technically, anyone testing PCR positive who dies in the next 28 days is classified as a ‘covid’ death. Mysteriously, deaths previously attributed to respiratory disease, influenza and pneumonia have gone down by about the same as ‘deaths from covid’ have gone up, when you compare all deaths, taking the month of July as an example, with the average over the past five years.
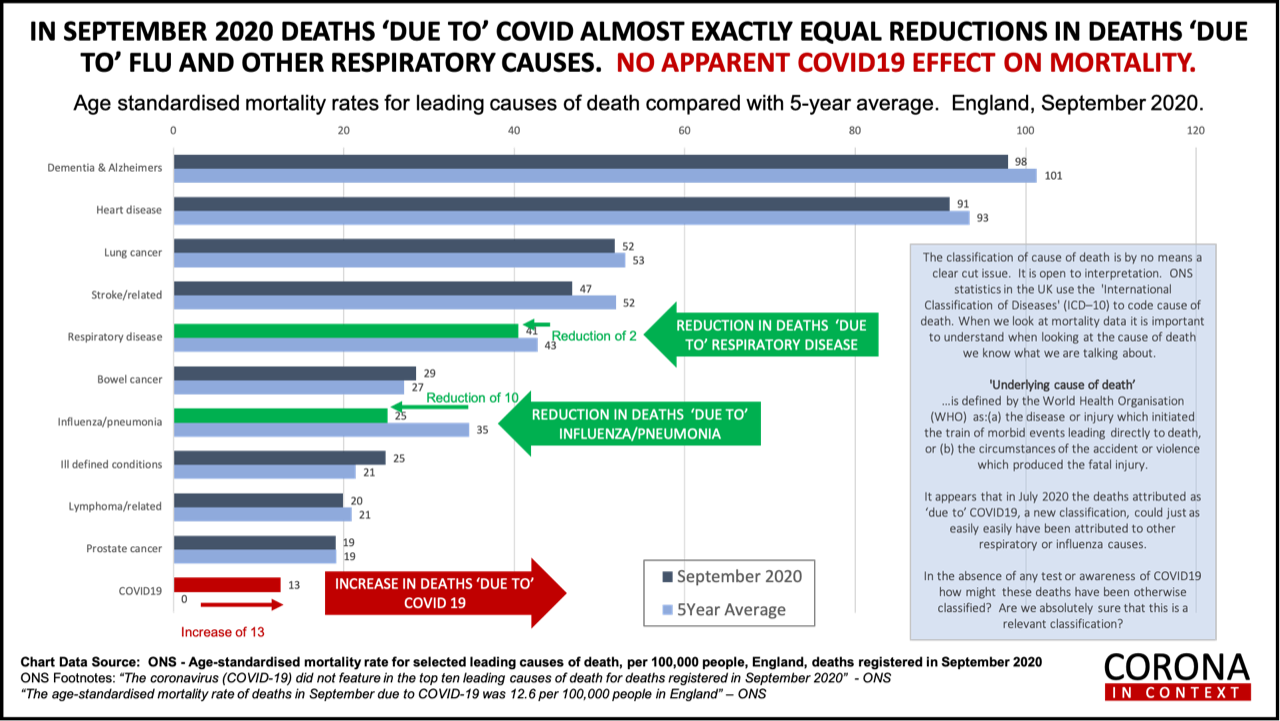
This morning, between 6 and 8am, my colleague Drew Fobbester did the same analysis on the latest, September data. Once again, the increase in apparent COVID-19 deaths seems to be coincidentally offset by the reduction in respiratory, flu and pneumonia deaths. (Thank you Drew!)
Even disregarding reclassifications less than half of one percent of deaths in August were attributed to covid.
A dozen or so hospital workers have told me that, in their hospital, anyone who dies of anything, but tests corona positive, even if they then test negative, are put down as a ‘covid death’ without further investigation. One hospital worker told me that no-one classified as a ‘covid death’ was actually investigated in any way. A real covid death produces a specific type of pneumonia (organising pneumonia) which can be seen in the nature of the lung tissue to confirm the actual case of death. Is this kind of ‘post mortem’ lung examination being done anywhere?
The vast majority of people who test positive either remain asymptomatic or have a mild illness, not dissimilar to a regular cold or flu. It has struck me that the ‘hardest’ measure of covid deaths would be from Intensive Care Units since that is where you go when critically ill. If, just for a minute, we put to one side care homes and the isolated elderly who might tragically die at home, if you or I got really sick we’d end up in hospital. Then, if our vital signs were crashing we’d be moved into the ICU. There’s plenty of capacity. Even in the height of the ‘first wave’ all ICUs in the UK were not full even though, in certain areas, they were pushed to the max. Right now ICUs are ready and waiting. If you think you’d end up in an ICU then this gives you a more realistic indicator of your risk.
YOUR RISK OF DYING IN AN ICU
With a total of 831,000 cases since 1st September and 314 ICU deaths that means that one person in 2,646 who tested positive died in an ICU.
With about 50 million adults in the UK (removing children from the population count) and, currently, 314 deaths in eight weeks and 140 deaths last week this means that your chances of dying this week is 1 in 35,417.
All these calculations of risks, of course, assumes you are neither supplementing vitamin DWhat it does: Helps maintain strong and healthy bones by retaining calcium. Deficiency Signs: Joint pain or stiffness, backache, tooth decay, muscle cramps, hair loss…., vitamin CWhat it does: Strengthens immune system – fights infections. Makes collagen, keeping bones, skin and joints firm and strong. Antioxidant, detoxifying pollutants and protecting against… or zincWhat it does: Component of over 200 enzymes in the body, essential for growth, important for healing, controls hormones, aids ability to cope with stress… and are in average poor health. I’m doing a full report on vitamin D and vitamin C in my November 100% Health Newsletter for subscribers to my 100% Health Club. As a general guideline, not an actual factual number, I would say that you have to be at least three times less likely to convert from ‘covid positive’ to bad enough to be hospitalised if your vitamin C and D levels are good, and, according to the Wuhan trial, 68% less likely to die in an ICU if you are given vitamin C. So you could, conservatively, divide your risk by at least 4, which means your risk of dying in an ICU from covid is about the same as being killed in a road traffic accident.
YOUR RISK OF A ‘COVID DEATH’ IF TESTING POSITIVE
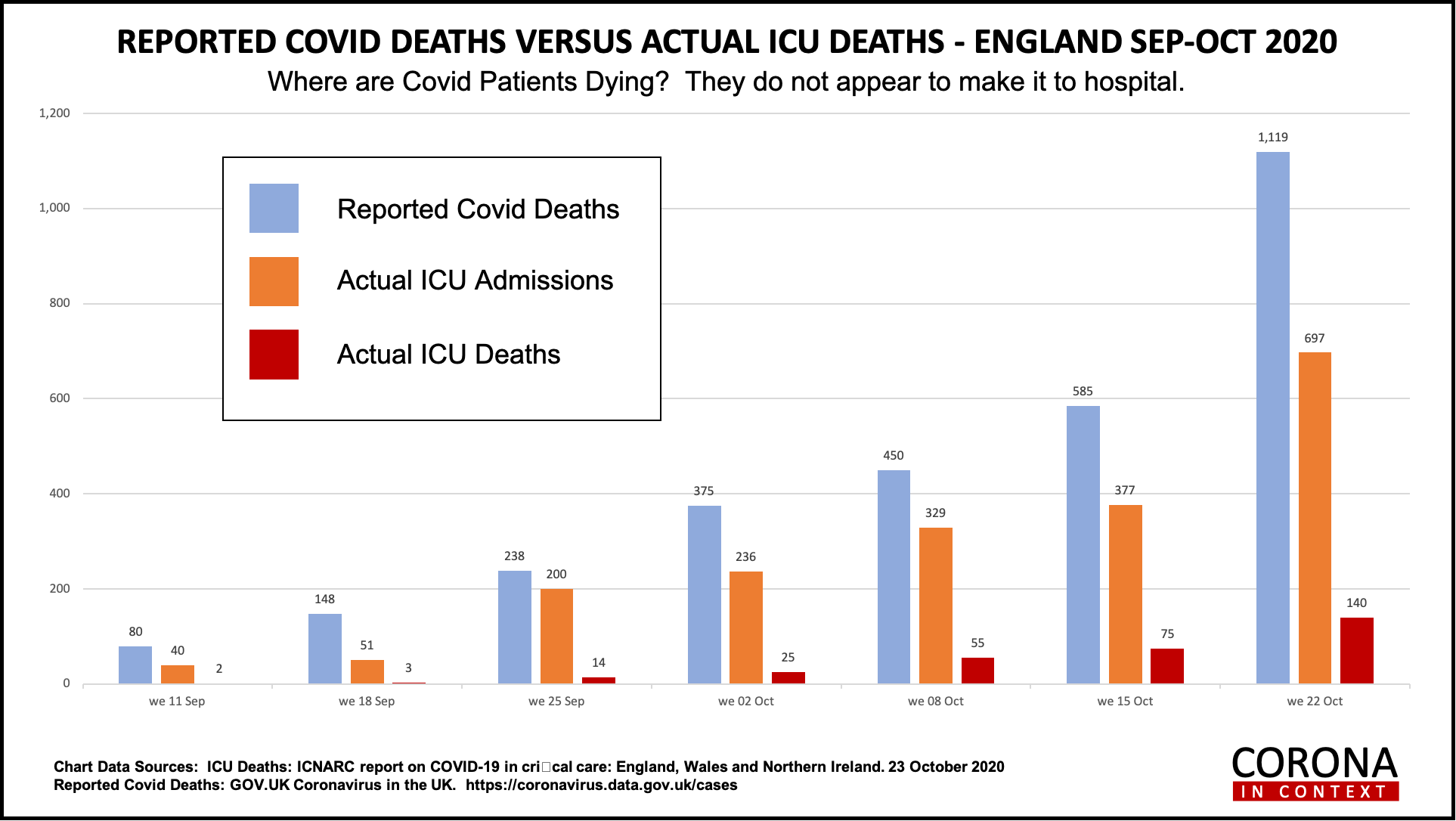
If, on the other hand, you take the government’s method of counting any death in anyone who has tested positive in the last 28 days then it looks like this. Last week (up to Oct 22nd) over two million tests were run (2,138,405) and 127,000 testing positive. That’s 5.9% testing positive. (If you deducted false positives it’s below 5% which the WHO say is the point below which lockdowns are not advised.) Let’s assume this rate applies to the whole nation and we had tested all 50 million adults you’d expect just shy of 3 million to test positive. [It will be less because more people tested are key workers or people who think they’ve been infected.]. Up to last week there were 1119 ‘covid deaths’. That means that about 1 in every 3,000 people tested die a ‘covid death’. There were 140 ICU deaths last week. Thus, assuming all were tested and 3 million were positive, then 1 in every 21,428 people testing positive die in an ICU.
Just to give us a further check on the validity of the ‘covid deaths’ there are eight times more deaths in this government figure than die in ICUs (taking last week’s figures eg 1119 deaths versus 140 deaths). Is that likely? Do you think 979 out of 1119 people don’t make it into an ICU within a hospital?
10,000 People Die Every Week: 1,252 from respiratory & flu
But please also bear in mind that even the alleged 1119 covid deaths in a week is very little when you factor in that around 10,000 people in the UK die every week, which includes approx 1,252 from respiratory deaths of which approx 500 are from flu [source: office for national statistics – and fullfact.org.]
Whichever way you analyse it, it looks pretty obvious that a significant proportion of so-called covid deaths are just deaths from flu or respiratory conditions, probably in people deficient in vitamin C and D, or other causes in people who just happen to test positive. Given that 44% of covid deaths are in nursing homes, where most flu deaths occur, if these poor people are dying of covid flu then that would explain why there are less left to die of other flu strains.
Whichever figures you believe in, if these odds are something you can live with then the point of social isolation and wearing masks is primarily to protect the vulnerable. That’s why the group of scientists who forms the Barrington Declaration say the current ‘lockdown’ strategy is wrong and doing more harm than good in the non-covid harms to people, such as the increase in mental illness. A survey by researchers from the University of Glasgow, based on a cross-section of over 3,000 adults reports that younger adults (18-29 years) were more likely to report suicidal thoughts – 14% of those from more disadvantaged backgrounds reported suicidal thoughts, and there are higher levels of depressive symptoms in those aged 30-59 years and over 60. One in four respondents experienced at least moderate levels of depressive symptoms. Then there’s the devastating impact on the economy and jobs.
This all suggests to me we should do what we can to build our immune resilience, protect the vulnerable by earing masks when around vulnerable people, but, otherwise, get on with life.
[SOURCES OF INFORMATION All cases and so-called ‘covid deaths’ come from the daily reports at https://coronavirus.data.gov.uk ; All ICU data and deaths come from the Intensive Care National Audit Research Centre (ICNARC).]
VITAMIN C DEFICIENCY IS RIFE IN ‘OVER 65 YEAR OLDS‘
Scurvy, caused by vitamin C deficiency, killed over two million sailors in the 17th and 18th century. Overt deficiency is defined as a vitamin C level below 11.4 µmol/l, while insufficiency is defined as below 23 µmol/l. An optimal level is around 100µmol/l. The average person in the UK has a level of 50µmol/l.
According to the the government’s ‘National Diet and Nutrition Survey‘ 4% of people over age 65 have overt vitamin deficiency., which equates to almost half a million people in the UK having levels of vitamin C seen in scurvy . This is partly because, the older you are the more vitamin C you need (cells become less efficient and make more ‘oxidant exhaust fumes’ with vitamin C has to detoxify) and partly because our diet is so poor.
These people, if they get virally infected, are unlikely to survive. How many deaths in the elderly and in care homes are a direct consequence of this widespread vitamin C deficiency? 
Last week I reported on a study of 21 critically ill COVID-19 patients admitted into an ICU in the US. The average vitamin C level of these patients was 22µmol/l which is low. The average level for 11 survivors was 29µmol/l compared to only 15 µmol/l for the 10 non-survivors with five (50%) below 11µmol/l. – the scurvy level. A study in an ICU in Barcelona of 18 COVID-19 adult patients found that 17 had undetectable levels of vitamin C. COVID-19, and all viral infections, deplete vitamin C rapidly. What really struck me about these results was that, while age is a risk factor for covid mortality, when the researchers factored in a person’s vitamin C level, age was no longer a predictor of mortality, but vitamin C was. This suggests that older people have lower vitamin C levels, and more need, and that’s what kills them.
Is this what’s happening in care homes? A survey of elderly Scottish patients hospitalized as a consequence of acute respiratory infections reported that 35% of patients had vitamin C plasma levels below 11 µmol/l. One study in a hospital in Paris reported that 44% of patients had vitamin C plasma levels less than 6 µmol/l, and in another hospital in Paris, 17% of patients had levels below 11 µmol/l. In a Canadian university hospital, it was found that 19% of patients had vitamin C plasma levels below µmol/l. In a study of surgical patients in Australia, it was found that 21% had vitamin C plasma levels below 11 µmol/l.
I think we should be testing our elderly and vulnerable for vitamin C and supplementing accordingly. Here’s the rub: there’s no vitamin C blood test on the list of tests that can be perfomed on the NHS in hospitals. I’ve found a vitamin C urine dipstick test that compares well to blood tests. We are trialling it in an ICU to identify who is deficient and needs more vitamin C. It’s cheap and seemingly accurate, but certainly should be good enough to identfy those clearly deficient and in need of vitamin C. I’ll let you know where you can get these urine vitamin C tests as soon as they become available just in case you know anyone in a care home or at risk.
[SOURCES OF INFORMATION: All studies referred to are referenced in the ‘Vitamin C for Covid’ review below.]
COMPREHENSIVE REVIEW ON ‘VITAMIN C AND COVID’ RELEASED
For the past couple of months I’ve been working on a comprehensive review entitled ‘Vitamin C – an adjunctive treatment for respiratory infection, sepsis and COVID-19’ with experts in vitamin C and leading professors of emergency medicine, public health and pharmacology. My co-authors include Associate Professor Anitra Carr from the Nutrition in Medicine Research Group, Department of Pathology & Biomedical Science at the University of Otago, New Zealand: Professor Iain Whitaker and Drs Thomas Jovic and Stephen Ali from the Institute of Life Sciences, Swansea University Medical School, Swansea University; Professor Paul Marik from the Division of Pulmonary and Critical Care Medicine, Eastern Virginia Medical School in the US; Emeritus Professor of Pharmacology, David Smith, from the University of Oxford; and we were greatly helped by Professor of Public Health, Harri Hemila from the University of Helsinki, Finland.
The review will next go through peer-review but is available for anyone to read at: https://www.preprints.org/manuscript/202010.0407/v1
Once it has been through peer-review and is published we will submit it to all relevant government and medical agencies calling for review of the evidence for vitamin C for covid and appropriate actions taken. If you’d like help in anyway to put vitamin C treatments into hospital, have our government and media encourage people to supplement vitamin C when under viral attack and remove the wrong classification of vitamin C for covid as ‘fake information’ in digital and other media please sign our petition at www.change.org/vitamin C4UK.
Stay healthy. Stay Free.

Comments
Join the Conversation on our Facebook Page