
Successful treatment has to do two things:
- reduce the rate at which people are dying
- make it less likely that infected people infect others (transmissibility).
The vaccine approach works in two stages. First by vaccinating the majority of the population a proportion of them will be less likely to develop the disease , reducing the death rate, and then ensuring that the rest are less likely to pass it on, at least for a while.
A vitamin approach works rather differently – it can still benefit people who do become infected. A population that has adequate vitamin levels will have fewer cases but if people are infected, a raised dose of the vitamin, given early, can cut the time they are infected and if the infection becomes serious, high doses can reduce the chances of dying. The result is that fewer people need treatment which is both more practical and more cost-effective.
Let’s see how these two scenarios might pan out with covid.
ASSUMPTIONS
Firstly, for the sake of comparison let’s agree on a few numbers to decrease the variables.
1. The first is that 2% of the population get infected and can transmit infection to others for 8 days. In the preliminary vaccine trials it was 1% over a period of months but, over time let’s assume this doubles. Right now, a little over 1% of those PCR tested are positive but a) this isn’t a random sample since many people get tested because they are symptomatic or have been in close contact with those who are and are worried and b) not everyone who is PCR positive gets symptoms; both because the test isn’t 100% accurate and because some people get infected but remain asymptomatic. According to Imperial College’s ongoing REACT study 0.51% are currently PCR positive. The ongoing ONS Coronavirus Infection Survey calculates one in 115, or under 1%. So 2% is probably towards a worst case scenario.
2. Secondly, the efficacy of a vaccine for preventing symptomatic infection averages out around 50%. So far, the range in relation to infection has been from 95% to 50% effective. The AstraZeneca vaccine was 70%. One dose of the Pfizer vaccine was reported as 50%, going up to 90%. But that was before the S.Africa and Brazil variants. The Moderna vaccine claims to be a sixth less effective against the S.Africa variant. There will be other variants, and, like the flu jab, the vaccines will be modified. The latest results reported in the press as an 85% reduced hospitalisation among those vaccinated versus unvaccinated, is probably a best case scenario since this was only seen in those vaccinated 28-34 days after vaccination. After 42 days the difference in hospitalisation dropped to 58% for the AstraZeneca vaccine and 64% for the Pfizer vaccine. However, for the age group of 18-64, in those who had been vaccinated 35-41 days beforehand, the difference in hospitalisation dropped to 43% then went up to 51% after 41 days from vaccination. This study is going through peer-review.
I suspect the actual efficacy in stopping someone from becoming symptomatic is likely to be around 50% plus or minus 20%, depending on one’s age and what variants come along. I’ve straw polled various vaccine scientists and they think this is a reasonable prediction. We don’t know, however, about the efficacy for preventing deaths.
In the Model below, based on the assumptions, vaccinating 100,000 people saves 50 lives, which is ten times more favourable than the preliminary trial results which showed one less death in 20,000 vaccinated. (However, if vaccination, for example, turned out to cut transmission on infection ten-fold this could be plausible.) This assumption would predict 25,000 lives if 50 million vaccinated so it’s pretty ‘bold’.
3. I’m also going to assume that half of those PCR infected end up in hospital. This is almost certainly an over-estimation because some remain asymptomatic, some get minor symptoms while some could tip into more serious COVID-19 requiring hospitalisation. According to a Nature journal article ‘research early in the pandemic suggested that the rate of asymptomatic infections could be as high as 81%. But a meta-analysis published last month1, which included 13 studies involving 21,708 people, calculated the rate of asymptomatic presentation to be 17%.’ Most have a mild infection not requiring hospitalisation.
4. My next assumption is a third of those hospitalised for COVID-19 end up in ICUs. The reason for these assumptions are a) in two trials on vitamin DWhat it does: Helps maintain strong and healthy bones by retaining calcium. Deficiency Signs: Joint pain or stiffness, backache, tooth decay, muscle cramps, hair loss…. (see below) 50% and 21% respectively of the control group receiving standard care, but no vitamins, ended up in ICUs. That averages out at about a third of hospitalised patients being admitted to ICUs.
5. The UK average mortality rate in ICUs not using vitamin CWhat it does: Strengthens immune system – fights infections. Makes collagen, keeping bones, skin and joints firm and strong. Antioxidant, detoxifying pollutants and protecting against… or D is around 30%. In other words, 70% in ICUs survive.
THE VACCINE MODEL
So, if 100,000 people are vaccinated, with 100% efficacy, 2,000 (2%) who would have got infected/symptomatic would be protected. But with 50% efficacy 1,000 would be protected and 1,000 would get COVID-19. Half of these, 500 people, end up in hospital, a third of which (167) end up in ICU and 30% die. That’s 50 deaths.
The second criteria is passing on infection. At this stage we don’t know if vaccinated people are able to pass on infection, or for how long. According to the Medicines Health Regulation Authority, who approve the vaccines for experimental use “The study data submitted to MHRA to date do not show that “the vaccine will not prevent recipients from being infected with SARS CoV-2 thus becoming infectious.” This fact is not at all widely known. Most people assume that if you get the jab your will become less infectious, but currently there is no data to support this.
But let’s assume that if your immune system is working well and you are infected, you will be infectious for a couple of days with minimal symptoms and then recover.
THE VITAMIN MODEL – STARTING WITH C
Now let’s take a look at vitamin C and D with the dynamics of each being somewhat different. Let’s start with vitamin C, which has three opportunities for an effect.
The first is if people take it every day, they will have decent levels if they are infected. The second is that they then take reasonably high amounts on the first day of infection and until they are symptom-free. The third is in hospital in the critical covid phase.
The clearest evidence for vitamin C is what happens if you take a high dose, say 8 grams, on the first day of an infection. In all studies to date, the more supportable prediction is that 6-8 g/day doses would shorten the duration of viral upper respiratory infections by 20%2. In the recent JAMA study, admittedly giving vitamin C to outpatients, in other words a few days after the start of an infection, the duration to recovery was reduced by 18%. A 20% reduced duration turns a 6 day symptomatic infection into a 5 day infection and, with a likely contagious pre-symptom day, that’s 6 days of transmissibility.
It may be better than this (especially if people took even higher doses). In one study giving 8 grams across the first day of infection 46% are symptom-free within 24 hours. If a higher percentage, let’s say 75%, were symptom-free within 2 days, then that also cuts down the length of time an infected person could infect someone else.
In this scenario one could be contagious for 3 days. So, vitamin C treatment could mean somewhere between 3 and 6 days transmissibility. So, a vitamin C treated person, if infected, could infect something like twice as many people as a vaccine treated person, assuming 4.5 days transmissibility.
One plus for the vitamin approach is that if, out of that 100,000 people only 2,000 become infected you have to treat far fewer people – only the 2,000 while you have to vaccinate the full 100,000 people.
The big unknown is the number of people who don’t get better and go on to develop critical covid. Let’s assume the vitamin C works for 3 in 4 – one quarter can still go on and develop critical covid.
So, from our 2,000 people who become infected and are treated or treat themselves with vitamin C, 500 end up in hospital. Let’s assume, again, that if given 6-8g a day on arrival, which is the dose those hospitals using vitamin C and reporting the lowest mortality recommend, let’s assume that 20%, not the usual third, end up in ICU. That’s 100 people.
Then, there’s the critical care end. The best results in ICUs have been with 3 grams every four hours (12g a day) given intravenously. Together with other medication, this has reduced mortality below 7%. In the Wuhan intravenous vitamin C study, giving 24g to ventilated patients, mortality was more than halved, and reduced by 80% in the most critically ill. These people were not getting steroids. It is reasonable to assume that, if given 12g plus other medication, mortality would be reduced from the current average of 30% to 10%.
So in our group of 100,000 people, 2,000 become infected and are given vitamin C. One quarter, 500, develop critical covid and are hospitalised. Of those 500 treated with high dose vitamin C in hospital, 20% or 100 end up in ICU and 10%, that is 10 die. That’s better than what you’d expect with vaccines.
VITAMIN D
Then there’s the vitamin D factor. We know that people with a higher vitamin D blood level have less chance of developing infection and, like vitamin C, if they do, would presumably recover more quickly.
It’s a hard figure to put a number on but we do know that countries close the equator, with vitamin D blood levels above 75nmol/l have much less covid infections and deaths. Ghana, with average vitamin D level of 76nmol/l for example, has 2,430 covid cases and 17 deaths per million compared to the UK which has 59,432 cases and 1,724 deaths per million, according to Worldometer. Studies also show that those with levels above 75nmol/l up to 100nmol/l are half as likely to test positive as those below 50nmol/l3. In winter half the UK population are below 50nmol/l.4
Unlike vitamin C, which works immediately, supplemental vitamin D takes a few days to be converted into the form that works in the body, so it makes more sense to pre-dose with vitamin D than to just take it on infection. Much like high dose vitamin A for measles, since it is stored in the body it doesn’t need to be taken every day. Even monthly would work, but weekly is probably better, and as good as daily.
Ideally, here, one would measure everyone’s vitamin D level and dose accordingly. This has a cost and some practicalities to overcome, but is not impossible. The goal would be to get everyone’s vitamin D level above 75nmol/l. Supplementing 3,000iu a day, or 20,000iu a week should achieve this. Testing is ideal but, alternatively, just give everyone a 20,000iu weekly supplement. This could reasonably be expected to halve symptomatic infections.
So, if we treat 100,000 people with vitamin D, 1,000 instead of 2,000 become infected. That’s halved the transmissibility. If the untreated transmissibility is 8 days then you could say this equates to 4 days, or close to what you’d expect with vitamin C treatment and worse than vaccination. (Half have no transmissibility, half have 8 days transmissability, so the average for the whole is 4.)
Of those 1,000 people who become infected half, that is 500, end up in hospital. On arrival in hospital they are given the hormonal form of vitamin D, calcifediol. We have two studies now that give us a good model of what happens next.
In the Castillo study only 2% ended up in ICU and none died5. In the recent Barcelona trial 5% ended up in ICU and 6.5% of those died6. Using the higher of these figures, of our 500 in hospital 25 end up in ICU and 2 die. That’s a lot better than the 50 deaths we’d expect in the vaccine model.
VITAMIN C AND D COMBINED
We can’t assume you can just add together the vitamin C and vitamin D benefit since they may both work on shared aspects of improving protective immunity. In other words, you can’t optimise immunity twice. But let’s assume there is some additional effect. NOT 2+2=4 but 2+2 = 3. So, if vitamin C cuts transmissibility from 8 days to 4.5 days (3.5 days less) and vitamin D from 8 days to 4 days (4 days less) the addition would be 7.5 days less, or under a day. Let’s double that to 2 – the same as the vaccination example.
Model based on 100,000 people treated
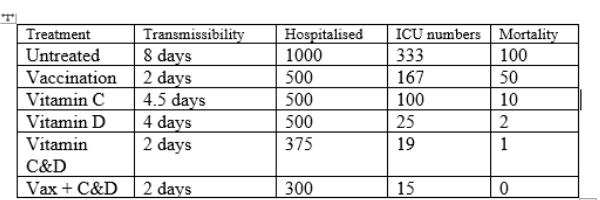
In relation to hospital admissions if both vitamin C intake from the start of infection and adequate vitamin D levels halve the chances of ending up in hospital let’s not halve the numbers down to 250, but split the difference to 375. Same with ICU numbers, to 19 and deaths to 1.
Even if these numbers are wildly optimistic and we halve the projected benefit, eg made every prediction twice as bad it’s still better than the vaccine model, or, at least surely worth considering. Alternatively, halving the benefit would also be realistic if you could only get half the population complying. (The same applies to vaccination.)
However you do the numbers it’s hard to see how a vitamin-led approach would not lead to less hospitalisation, less ICU admissions and less deaths than a vaccine-only approach, thus taking the burden off the NHS and medical system.
Also, for those who are vaccine hesitant the vitamin approach may be attractive to them and has the knock on effect of protecting others.
You can, or course, do both. The combined figures above are very conjectural but the idea that your strengthen your immune system both by inducing a fast antibodyAn antibody is a protein produced by the body’s immune system when it detects a harmful substance known as an antigen. Examples of antigens include… reaction with the vaccine and a strong immune response due to vitamin C and D makes sense as a ‘belts and braces’ approach.
One could also add in zincWhat it does: Component of over 200 enzymes in the body, essential for growth, important for healing, controls hormones, aids ability to cope with stress…. I haven’t because there’s not enough studies to guess at the numbers. However, studies giving 70mg+ upon infection have cut duration of infection by a third. That would both reduce transmissability and reduce the percentage of people ending up with severe covid. Zinc has been shown to be low in COVID-19 patients. Also, a couple of studies giving 50-100mg of zinc have shown better outcomes including less deaths, but they are usually combined with hydroxychloroquine, which helps get zinc into cells, so it’s a bit ‘muddy’. On a practica level I’d certainly recommend supplementing at least 50mg, ideally 70mg of zinc during a viral infection spread out across the day.
In reality, by July, most people will have been vaccinated so the real question here is should the vitamin approach be added on? From a research point of view it will be really interesting to compare those vaccinated to those unvaccinated, taking vitamin C, D and zinc, to get a real-life comparison. We need a number of nutritionally aware, vaccine hesistant people to do this.
COSTS & PRACTICAL ISSUES
The vitamin-based approach has certain costs and practical issues.
1. You’ve got to get everyone, or at least everyone with low levels, taking a high dose vitamin D supplement once a week during winter or this pandemic. There are issues of supply, cost and distribution. (There could be a vitamin D and C subsidy for collection at pharmacies and health food shops.)
2. You’ve also got to make sure everyone has an immediate supply of 8 grams of vitamin C a day upon infection. A pot of 60 1 gram tablets is a week’s supply at this dose and the retail price is around £5. If the government bought by the ton, as they did in China, it would be much cheaper.
3. Then the hospitals have to give it out orally to those able to swallow and intravenously for those more critically ill. The savings in length of stay of hospital or ICU stay would far outweigh the costs. Already, there is evidence that both vitamin C and D reduce length of time in hospitals, ICUs or on ventilators. Since some ICUs are doing this already we can assume this is not only doable but cost-saving, not cost-incurring.
4. Then you have the issue of compliance. One assumes they’ll be some anti-vitaminers. But we’ve all seen how effective the Government and media have been in instilling the idea that everyone must be vaccinated. If vitamins had a similar non-stop media push and promotion would we achieve 80% compliance? I’d think so because if vitamins are shown to work they don’t have the same perceived potential downsides of vaccinations, whether true or not. No-one has ever died from taking a vitamin supplement. There’s a persuasive ‘why not?’ argument.
The vaccine-based approach has it’s own costs and practical issues.
1. Firstly, you have to vaccinate everybody. The total cost probably works out around £20 to £30 per person when you factor in staffing. If anyone has a good figure for it is costing let me know.
2. On the downside, while there is no known safety risk with this kind of vitamin C and D strategy, there potentially is with vaccines. This requires another layer of ‘support’ costs – including medical costs and pay-outs for a small percentage of people who are damaged by a vaccine. This happens. If this were one in 10,000 in our model population of 100,000 people it would be 10. If it were one in 100,000 it would mean one person needing compensation, or 500 in 50 million. The Government have indemnified the vaccine makers and set a maximum payout of £120,000. Paying out 500 vaccine-damaged people would cost £60 million. This is a very hard cost to even predict at this stage, and no doubt very contentious, but it is certainly worth bearing in mind. Red flags already exist for the Pfizer vaccine in the US with one third of deaths reported to the US Center for Disease Control occurring within 48 hours of vaccination. So far in the UK up to Feb 14th, there have been 58,250 adverse reaction ‘yellow card’ reports , roughly one in 260 people vaccinated, including 402 fatalities and many significant disabilities. Now, how many of these are triggered by the vaccine is a different question but for a ‘yellow card’ report to be raised that means the doctor considers the association questionable. The true figure will be higher, possibly by a factor of 10, as generally a small percentage of adverse reactions get reported. I’m not aware that a ‘yellow card’ fatality has ever been reported for vitamin C or D, just to put this in context.
3. Then you have compliance. At the moment it is looking like 80% vaccination compliance might be achieved.
Even though there are grounds to challenge many of these assumptions it does, at least, provide a starting point or a framework for looking objectively at these options. As new studies are published assumptions can move closer to a likely reality. The model can evolve and improve.
However, I hope you will agree that it no longer makes any sense at all to not include vitamin C and vitamin D in the overall strategy and treatment protocol for COVID-19.
COVID RESULTS LAST MONTH – FROM THE FRONTLINE
Every month I’ve reported what’s been happening week by week in Intensive Care Unit who record COVID-19 deaths most accurately because the diagnosis of a critical COVID-19 case is much less ambiguous than the ‘deaths within 28 days of a positive PCR test’ which is a mixed bag of people dying of covid and dying of something else but with covid positivity. The chart below shows both, and also admissions into ICUs across the UK since September 1st. Covid deaths in ICUs averages out at 14% of the total of ‘covid positive deaths within 28 days’. In other words, for every one person who dies in ICUs six die elsewhere, eg 4 in hospital and 2 at home.
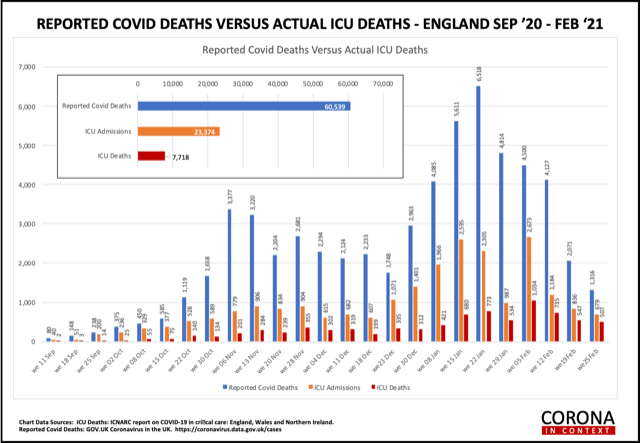
Based on the pattern of flu deaths one would expect January and February to be the worst months. So, hopefully, the trend towards less admissions and deaths and less covid-related deaths overall will continue to decline. What you’ll see in the chart is that ‘PCR positive covid deaths’ have declined alot, new admissions to ICUs have also declined but not so dramatically. The percentage of deaths appears higher but this is a legacy of the previous high admissions.
What’s contributing to the overall decline in covid deaths and ICU admissions is a hard one to tease out. There’s the potential knock on effect of locking down and also of vaccination. What is a bit strange is that, while the recent study going through peer-review shows there has been between an 85% and 43% reduced hospitalisation in those vaccinated versus unvaccinated up to 8th Feb, given that almost all of the 80+ age group have been vaccinated you’d expect a relatively greater decrease in mortality in those in this age, compared to other age groups that haven’t been vaccinated. There is no sign of this happening. The pattern of 28 day mortality across age groups hasn’t changed.This is not shown in the chart above but is in the weekly ICNARC reports that I receive.The ultimate test of vaccination working has to be the decrease in deaths of those vaccinated versus unvaccinated.
If COVID-19 deaths continue to decline through March and April, which is what you’d normally expect as sunlight returns (think vitamin D) and temperature increases people will speculate as to whether this is due to lockdown, vaccination and a drop on the R number, or seasonal effects. Therefore, it will be very helpful to monitor a similar group of non-vaccinated people versus vaccinated people to see if deaths and infections decline in one group more than the other. This is, in effect, the continuation of the vaccine trials and is happening. Those in the control group are being ‘unblinded’ and given the vaccine so we can expect reports in the next month or two. Ironically, we need some vaccine hesitant people to not be vaccinated to be able to do the research.
I hope more and more people are supplementing vitamin C and D as well as zinc. This information also needs to be collected so we can start to test this model and see if people doing one or the other or both have different levels of infection and mortality. The Big Data Institute at the University of Oxford has access to NHS records of vitamin D levels in those tested. This is an obvious way to see what the difference there has been in rates of infection and deaths according to vitamin D levels or prescribed supplementation.
If COVID-19 fades away, which I sincerely hope it will, as many viral pandemics seem to after the second wave, all this learning may be too late for COVID-19 but provide us with more viable solutions for the future.
Meanwhile, there is something we can all do now on the nutrition front to increase one’s odds and reduce transmissibility and that is:
• Test your vitamin D level and get it above 75nmol/l, ideally at around 100nmol/l. You’ll probably need to take 3,000iu a day in these winter months to achieve this.
• Take 2 grams of vitamin C a day and have a good supply, as well as zinc, in the event you get any cold/covid symptoms.
References
1. C. Sudfeld et al., ‘Effectiveness of measles vaccination and vitamin A treatment’
International Journal of Epidemiology, Volume 39, Issue suppl_1, April 2010, Pages i48–i55, https://doi.org/10.1093/ije/dyq021
2. https://doi.org/10.1002/14651858.CD000980.pub4 https://helda.helsinki.fi/handle/10138/225864; see also https://doi.org/10.3390/nu9040339; see also https://doi.org/10.1016/0895-4356(96)00189-8 https://doi.org/10.1016/0895-4356(96)00191-6; see also https://helda.helsinki.fi/handle/10250/8082 https://helda.helsinki.fi/handle/10138/225873; see also https://www.mv.helsinki.fi/home/hemila/H/HH_1996_JCE.pdf; see also https://www.mv.helsinki.fi/home/hemila/H/1996_L_JCE.pdf; see also https://doi.org/10.3389/fmed.2020.559811
3. Meltzer et al. JAMA Netw Open. 2020;3(9):e2019722; D’Avolio, A., et al. (2020). Nutrients 12(5)
4. https://www.nice.org.uk/guidance/ph32/documents/expert-paper-3-vitamin-d2
5. Entrenas Castillo, Marta et al. “”Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: A pilot randomized clinical study”.” The Journal of steroid biochemistry and molecular biology vol. 203 (2020): 105751. doi:10.1016/j.jsbmb.2020.105751
6. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3771318#
Comments
Join the Conversation on our Facebook Page