

To get the ball rolling back in 2020 myself and a group of experts, most members of the Scientific Advisory Board of vitaminC4covid.com, a not-for-profit initiative supported by over 1,000 medical and nutrition health practitioners and scientists, wrote a review entitled “Vitamin CWhat it does: Strengthens immune system – fights infections. Makes collagen, keeping bones, skin and joints firm and strong. Antioxidant, detoxifying pollutants and protecting against… – an Adjunctive Therapy for Respiratory Infection, Sepsis and COVID-19” This was published in the leading journal, Nutrients in December 7th. It cited over 120 studies, established vitamin C’s remarkable safety even at high doses, and has had over 20,000 downloads and not one critique. It makes the case for vitamin C for covid, both in prevention and treatment, undeniable. This review was/is ‘noted’ by the above organisations but has not been acted on.
In their defence, back in December, there had not been actual ‘intervention’ trials, but what you could call circumstantial evidence such as the high incidence of vitamin C deficiency in those dying of covid and that patient’s vitamin C levels predicted their survival. Most dying had scurvy levels of vitamin C as a consequence of unresolved viral infection.
But then the intervention, prevention and observational trials of covid patients given vitamin C started to be published and, as they did, we circulated them to all these agencies. The first, a randomised-placebo controlled trial in Wuhan ICUs, giving intravenous vitamin C for 7 days, reported a 70% reduced hospital and ICU duration and an 80% reduction in mortality in the most critically ill ventilated patients, plus improved oxygenation and reduced inflammation in all covid patients given vitamin C. These results were statistically significant1 and much better than the 30% reduction in mortality in ventilation patients seen in the dexamethasone recovery trial.2
Then a trial giving less critically ill covid outpatients 8 grams of oral vitamin C versus placebo showed an improved recovery rate of 70% – better than any anti-viral drug tested to date.3 The trial’s abstract, in the Journal of the American Medical Association, obfuscated this positive result.4
There are now seven other trials and all bar one has shown vitamin C to be effective with, broadly speaking, the higher the dose and the longer the treatment the greater effect. We are currently writing a review paper combining all studies. This is what our government agencies should be doing but are they?
Why is Public Health England reluctant to disclose any vitamin C review?
SACN had told us they’d review the evidence in their June meeting. It now appears, in their March meeting minutes obtained through a Freedom of Information request (FOI) they were instructed not to. As Jo Churchill says “SACN will not be duplicating work of other organisations and will therefore exclude studies focusing specifically on vitamins C and D, as these are being undertaken as part of the RAPID-C19 initiative.”
This is bizarre since, as she says “SACN is monitoring emerging evidence of nutrition and immune function specifically in relation to COVID-19. SACN’s remit is to assess risks and benefits of nutrients/foods to health by evaluating published scientific evidence and, based on its assessment, make dietary recommendations for the UK’s general healthy population.” Is there anything more important in the field of nutrition right now than to assess the role of vitamin C and D status in reducing incidence, duration and severity of covid? Why have our neighbours, Ireland, told its public to supplement 1,000ius of vitamin DWhat it does: Helps maintain strong and healthy bones by retaining calcium. Deficiency Signs: Joint pain or stiffness, backache, tooth decay, muscle cramps, hair loss…. daily all year round for this very reason?
The point is, as she says, “SACN has a public health focus and the treatment of disease is therefore outside its remit” but when does a vitamin deficiency that increases likelihood and severity of a disease stop being a public health issue and start being a ‘treatment’ issue? The whole point of separating NHS England, treating disease, and creating Public Health England (PHE), was to prevent disease. Does vitamin C not do exactly this this? By stopping covid positive people developing severe symptoms that need hospitalisation and treatment is vitamin C not potentially doing exactly what PHE was set up to do – take the burden off the NHS?
So, we issued an FOI on PHE/SACN to disclose their June meeting minutes, which they had been promising was the time vitamin C would be discussed. PHE’s reply states: “It is in the public interest to withhold the information in line with the publication schedule, so the information is accessible to the wider general public at the same time”. We’ve now issued an FOI to get this ‘publication schedule’. A year and a half has passed since covid struck in the UK and still no statement on vitamin C. Jo Churchill says “Based on the data currently available, we do not believe that there is sufficient evidence at this stage to conclude that vitamin C is a safe and effective treatment for COVID-19.” It implies that PHE, advised by SACN, has reviewed the evidence, but have they? Can we see it? Apparently not. Vitamin C is actually safer than water and all studies confirm this including a study of 9,328 patients given an average intravenous dose of 24 g of vitamin C every 4 days, primarily for cancer, infection or fatigue, reported that 101 (1%) had side effects, mostly minor, including lethargy/fatigue, a change in mental status and vein irritation/phlebitis5. Remember, these are sick patients, most with advanced cancer.
How slow is RAPID C19?
You may recall calls for more transparency of who was actually in SAGE (the Scientific Group for Emergencies) advising on covid strategy. This then morphed into NERVTAG (New and Emerging Respiratory Virus Threats Advisory Group). We could, at least, find a list of their members and supplied them with all the evidence for vitamin C – with zero response. Well, it’s morphed again into RAPID C19 (Research to Access Pathway for Investigational Drugs for Covid-19) under the auspices of NICE (National Institute for Clinical Excellence). It’s described by NICE as ‘a multi-agency initiative to ensure safe and timely patient access to treatments that show evidence of benefit in preventing and treating COVID-19’. Sounds like vitamin C would fit right in. We had, by the way, already supplied NICE with all the studies showing just how effective vitamin C was and asked them if they had or would review the evidence. They said that RAPID C19 was doing it.
So I contacted James Palmer, RAPID C-19’s National Medical Director employed by NHS England and NHS Improvement asking if they had reviewed the evidence for vitamin C. He replied saying “To date, RapidC19 considers that there is insufficient evidence to recommend Vitamin C for roll out as a potential routine therapy for patients infected with COVID-19, but will continue to keep this under review.’ I replied asking to see their assessment to support this statement. He replied saying “These assessments are held by NICE.”
I responded saying ‘NICE have never replied, never done a review, or at least shown one, and someone in their contact team passed us on to RapidC19, hence yourself. When you say ‘To date, RapidC19 considers that there is insufficient evidence to recommend Vitamin C for roll out as a potential routine therapy but will continue to keep this under review.’ it suggests that RapidC19 has actually reviewed the evidence. Are you telling me that RapidC19 haven’t and rely on NICE, who also haven’t?
Our request is very simple – if either RapidC19 or NICE have actually done of review of the evidence for vitamin C for COVID-19 can we, as members of the scientific and medical community, see it?’
I am reminded of one of those football games where the ball keeps being passed from player to player, backwards and forwards, but no-one scores a goal. PHE say SACN advises them. SACN say they been told to drop the vitamin C ball and pass to RAPIDC19. RAPIDC19 kicks it over to NICE. NICE passes it back to RAPIDC19. There’s certainly a whole lot of duck and diving going on.
So, we issued a FOI request on NICE and RAPIDC19. They responded, after considerable delay explained by numerous holidays, with a ‘briefing on vitamin C’ document dated 9th September, 2020 – almost one year ago. It states that “Vitamin C (ascorbic acid) has potential benefit in patients with severe and critical COVID-19 because these patients are likely to experience oxidative stress or severe inflammation.”… “There is only 1 published randomised controlled trial investigating ascorbic acid injection reporting preliminary results. This shows no significant difference in 28-day mortality or ventilation outcomes, however this trial is still recruiting.” This was referring to the Wuhan trial. There’s then a link to an appendix which says “the vitamin C group showed a significant reduction in 28-day mortality (p=0.05) in more severe patients. The significance was lost after adjustment (p=0.06,)” it also says that the vitamin C patients had a steady rise in oxygenation (p=0.01) and reduction in inflammation (p = 0.04).
Those in medical science will know that ‘p’ is the probability that the result is real and not random. Anything equal to or less than P=0.05, which means in layman’s terms that if you ran the same experiment 100 times you’d expect this result 95 times, is usually considered statistically significant. When the Wuhan trial was published, in December, the 80% reduction in mortality in the most critically ill ventilated patients had p=0.04. Of course, RAPIDC19 know this because we sent them and NICE the paper with the relevant sections highlighted. Less death, less inflammation, improved oxygenation – all statistically significant. This compares to the dexamathasone trial where the ventilated patients were 30% less likely to die.
The RAPIDC19 September briefing also states ‘There is currently no evidence indicating any signal of harm.’ So where is Jo Churchill getting her information from to state that there is insufficient evidence that vitamin C is safe?
In this briefing RAPIDC19 also state that ‘there are 14 ongoing randomised trials; 13 for treatment of COVID-19 and 1 in the prevention of COVID-19. 1 randomised trial with a target enrolment of 140 patients has reported early results (the Wuhan study). The ongoing prevention study is a randomised double-blind study of healthcare workers with a target enrolment of 600 patients (the JAMA 8g vitamin C for outpatients study); and 8 ongoing trials investigate vitamin C injection, 1 trial investigates oral vitamin C and 8 trials do not state the vitamin C formulation.’
So, back in September, they list the studies underway to watch out for, eight of which have been published, seven of which show clear benefit. Have they really not reviewed them? We have, after all, supplied the papers. So, we issued a further FOI request for any such review or statement since September last year. So far, no response.
Double Standards for Drugs and Vitamins
Never mind anti-vax are we seeing evidence of anti-vits? Given that vitamin C has no safety issues and is also part of the body’s natural biochemistry with multiple beneficial immune, antioxidantAntioxidants are substances that protect cells within the body from damage caused by free radicals. They help to strengthen the body’s ability to fight infection… and anti-inflammatory effects surely the bar to its use should be set lower not higher? The reverse seems to be the case.
Yet less effective anti-viral drugs such as Ronapreve (Regen-Cov in the US), which reduced the risk of death by 20 per cent in a subset of hospitalised patients, are being licensed for covid with much less evidence of benefit, more adverse effects and considerably more cost, with each dose costing £ £1,500. 6Bear in mind that the usual process in medical science is someone other than the company who makes the drug runs a trial. That has not yet happened with the vaccines, and safety trials are far from complete which is why vaccines remain unlicensed.
One argument given by Government is to wait for the results of the UK’s only participation in a vitamin C trial, namely REMAP-CAP. This is a trial that several ICUs are signed up for, giving critical covid patients either vitamin C or placebo added to standard treatment. Personally, I think at this stage of evidence it is unethical to deprive any critical covid patients of vitamin C. For this very reason leading ICUs such as the Chelsea and Westminster Foundation who already give vitamin C have refused to participate. But there is the very real possibility that REMAP-CAP is designed to fail by giving vitamin C for only 4 days. The reason this is too short, as it would be for steroids or antibiotics, is that you don‘t stop a life-saving treatment in a patient hovering on the edge of death until they are out of the woods. Withdrawing vitamin C, steroids or antibiotics too soon can trigger a worsening on symptoms. Now, if you measure results on day 10 that would obscure a positive effect, but if you measure results on day 4 that should still count.
But the biggest issue with REMAP-CAP is that it hasn’t started. According to the RAPIDC19 briefing in September ‘the RAPIDC19 vitamin C arm is closed’ due to lack of vitamin C supplies! The suppliers, however, never ran out. It meant that non-one got the vitamin C treatment in the second wave. Now, they say, vitamin C supplies are available so, hopefully, some will get treated in the third wave if there is one. In her most recent letter to MPs Jo Churchill says ‘The REMAP-CAP trial into vitamin C started recruiting in November and we expect recruitment to increase. This is dependent on the number of patients in intensive care.’ This is a considerable stretch of the truth because ICUs we followed up in June hadn’t treated a single person – and you can’t recruit a critical patient without having vitamin C. Is this a delay tactic?
My view is that all this anti-vitamin institutional caution and trial delays is a form of irresponsible recklessness that has, and is costing, thousands of lives. Never mind a third wave, we need a third way based on supporting natural immunity, not just the current two pronged strategy of avoiding transmission with lockdowns, masks and tracking and vaccinations.
March on Saturday 28 August
Join us in a march to raise the profile of Vitamin C for COVID on Saturday 28th August. Meet at 12:30pm at Hyde Park Corner – in the middle by the Royal Artillery Memorial.
THE MYTH OF HERD IMMUNITY
There are only two possible reasons to vaccinate children, who have little risk themselves. One is so they don’t infect the vulnerable and the other is to achieve herd immunity.
The former ignores the fact that vaccinated people still get infected, and infect others, albeit fewer because they are infectious for less time. The same, of course, applies to taking vitamin C upon infection, and having a good vitamin D level. Surely, that’s a better way forward for children given that the same risks of adverse reactions and deaths from vaccination apply to them but without the life-saving benefits? A University College of London study reports overall mortality rate of 2 per million children and a one in 50,000 chance of being admitted to an ICU, according to the BBC.7 A Kings College study reports that fewer than one in 20 (4%) were found to have experienced symptoms for four weeks or more, with one in 50 (2%) having symptoms for more than eight weeks.8
Please note that doctors have now made over 1,596 yellow card reports associating vaccination with deaths which is more than the 1,538 annual deaths from road traffic accidents in 2019. This comes directly from the gov.uk
The latter reason, to achieve herd immunity, is a myth as Dr Alexander Corbishley, senior lecturer at the University of Edinburgh in infections and immunity, points out in his letter in the Financial Times. It reads as follows:
“Published estimates of the proportion of the population that must be vaccinated to achieve herd immunity range from 60 per cent to above 90 per cent.
Herd immunity has a boring definition — it is one minus the reciprocal reproduction rate of R0. The Centers for Disease Control and Prevention estimates that R0 is 2.5, although this is likely an underestimate for the more infectious Alpha and Delta variants.
Using this estimate, 60 per cent of the population must be vaccinated to reach the point where the virus is unable to sustain itself within the population.
This however assumes that vaccines are 100 per cent effective at preventing transmission, which they are not. On Wednesday this paper reported that full vaccination halves transmission of the Delta variant. If this is accurate, then the proportion of the population that must be vaccinated to achieve herd immunity (assuming R0 of 2.5) is an impossible 120 per cent.
The inconvenient truth is that herd immunity against Sars-Cov-2 is a mirage. This should not come as a surprise. We have never achieved herd immunity for any coronavirus in any species. Why would Sars-Cov-2 in humans be any different? The most plausible end point is that we reach a state of endemic stability, where Sars-Cov-2 infections are common, but severe Covid is not. The sooner we stop talking about herd immunity, victory, defeating the virus or freedom from Covid, the faster we can come to terms with this reality.”
At the start of this pandemic I predicted 50% effectiveness for the vaccine, which my Oxford colleagues confirmed was likely and looks to be about right. The thing about natural immunity is that it offers robust protection against all variants, whereas vaccine-induced immunity can’t. The reason for this is because when you recover from the natural infection, you have both antibodies and T cells against all parts of the virus, not just the spike proteinProteins are large molecules consisting of chains of amino acids. Proteins are essential nutrients for the human body – they are a building block of…. That’s why vitamin C, D and zincWhat it does: Component of over 200 enzymes in the body, essential for growth, important for healing, controls hormones, aids ability to cope with stress… are so important as they support natural immunity.
ARE COVID DEATHS ACTUALLY RISING? IS THERE A THIRD WAVE?
Readers on my COVID NEWS will know that I’ve been tracking actual ICU covid admissions and deaths to give a true reflection of what’s happening at the sharp end. Here’s what actually happening up to last week.9
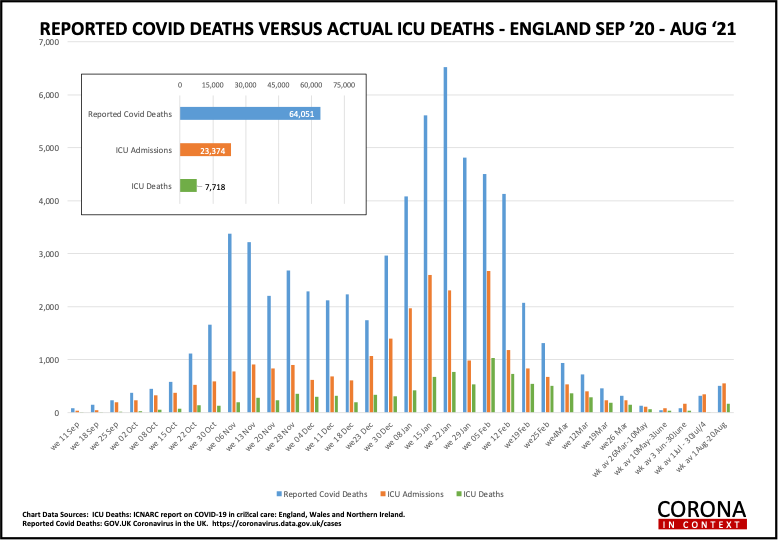
As you see there is a small, steady increase in ICU admissions and deaths up to a similar level seen at the end of the second wave back in late March. The percentage of people testing PCR positive (not shown on this graph) has increased from a low of 0.1% in June to 0.28%, which is slightly up from what was occurring in May (0.24%). If this were applicable to the whole population, bearing in mind that a proportion of people who are test often do you because they suspect infection, it means that 3 people per 1,000 are likely to be infected. The word from the hospitals that are using vitamin C etc is that they’ve learnt how to keep people out of ICU and treat them more effectively in hospital but there’s a small percentage of people, somewhat regardless of age, who do not respond to treatment and end up in ICU of which, for a national average, about a third do not survive.
References
1. Zhang J, Rao X, Li Y, Zhu Y, Liu F, Guo G, Luo G, Meng Z, De Backer D, Xiang H, Peng Z. Pilot trial of high-dose vitamin C in critically ill COVID-19 patients. Ann Intensive Care. 2021 Jan 9;11(1):5. doi: 10.1186/s13613-020-00792-3. PMID: 33420963; PMCID: PMC7794643.
2. RECOVERY Collaborative Group, Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, Linsell L, Staplin N, Brightling C, Ustianowski A, Elmahi E, Prudon B, Green C, Felton T, Chadwick D, Rege K, Fegan C, Chappell LC, Faust SN, Jaki T, Jeffery K, Montgomery A, Rowan K, Juszczak E, Baillie JK, Haynes R, Landray MJ. Dexamethasone in Hospitalized Patients with Covid-19. N Engl J Med. 2021 Feb 25;384(8):693-704. doi: 10.1056/NEJMoa2021436. Epub 2020 Jul 17. PMID: 32678530; PMCID: PMC7383595.
3. https://doi.org/10.21203/rs.3.rs-289381/v1
4. Thomas S, Patel D, Bittel B, Wolski K, Wang Q, Kumar A, Il’Giovine ZJ, Mehra R, McWilliams C, Nissen SE, Desai MY. Effect of High-Dose Zinc and Ascorbic Acid Supplementation vs Usual Care on Symptom Length and Reduction Among Ambulatory Patients With SARS-CoV-2 Infection: The COVID A to Z Randomized Clinical Trial. JAMA Netw Open. 2021 Feb 1;4(2):e210369. doi: 10.1001/jamanetworkopen.2021.0369. PMID: 33576820; PMCID: PMC7881357.
5. Padayatty, S.J.; Sun, A.Y.; Chen, Q.; Espey, M.G.; Drisko, J.; Levine, M. Vitamin C: Intravenous use by complementary and alternative medicine practitioners and adverse effects. PLoS One 2010, 5, e11414.
6. https://www.dailymail.co.uk/health/article-9872031/Drug-protect-10-dont-respond-Covid-vaccine-soon-available-NHS.html
7. https://www.bbc.co.uk/news/health-57766717
8. https://www.bbc.co.uk/news/health-58071898
9. https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting
Comments
Join the Conversation on our Facebook Page