In the last twenty years there has been no change in annual measles death rates, which hover between none and one a year, regardless of numbers of cases of measles. Cervical cancer deaths in the UK had been falling steadily since the 1970s, then started to level off in 2006-8, just before the HPV vaccine was introduced (see chart below – source Cancer Research UK).
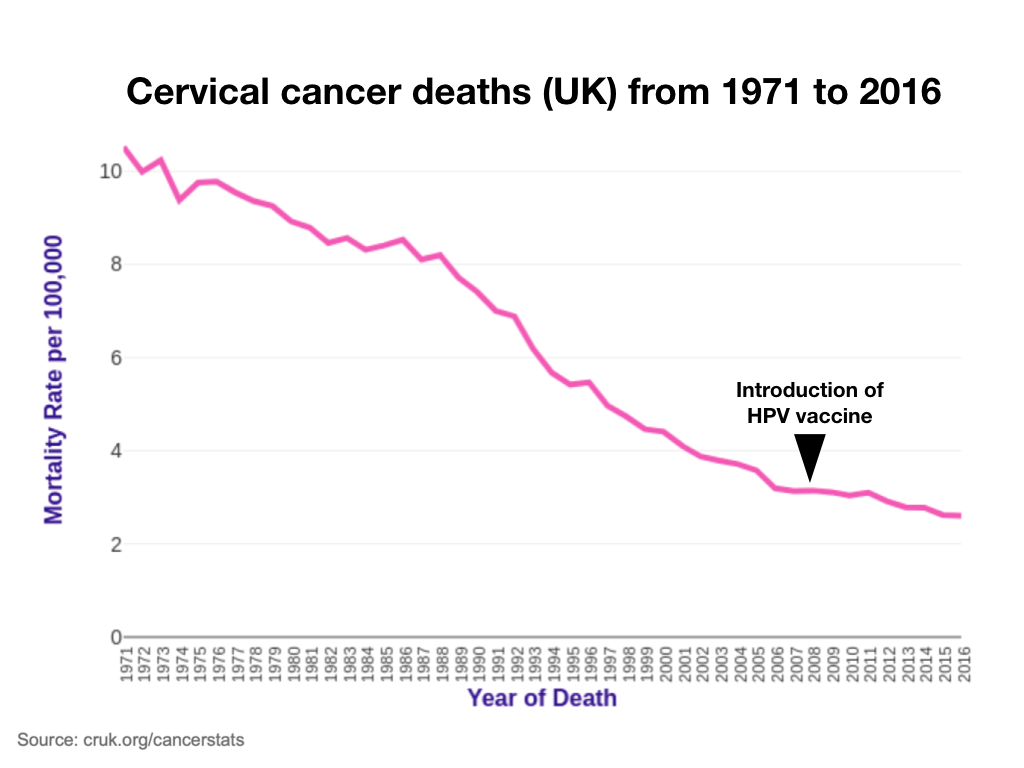
As of 2016 there’s no evidence of HPV vaccine has saved any lives, although maybe it will in years to come as cases of genital warts, the first sign of HPV infection, has reduced considerably. I’ve not been able to find a death from mumps or rubella this century.
A decade ago the Telegraph reported that “Eighteen babies and toddlers have died following childhood vaccinations in just four years, a secret Government report reveals.” Read the report for yourself. That would mean that, in these four years, more children died following vaccinations than have died from measles, mumps or rubella this century. In 2017 a report in the British Medical Journal highlighted the fact that, in Europe, as reported in the European Medicines Agency (EMA) database of adverse drug reaction reports were “275 deaths reported.. with acknowledgement that only approximately 10% of serious adverse events are reported.” Association doesn’t prove cause but doctors reporting these deaths do so because they are sufficiently concerned that the vaccine may have been to blame. Against the backdrop of circa 870 deaths a year from cervical cancer these are worryingly large numbers.
The argument is that you need 95% of the population to be immunised by a 100% effective vaccine. The MMR is much less than 95% effective. The mumps component is 65% effective after one dose, and 88% effective after two. The MMR, which hasn’t changed, remains controversial because of the autism link. The fact that a) an Italian court ruling that a boy’s autism was caused by the MMR and b) a US court ruled that Hannah Polling’s autism was caused by multiple vaccines and c) that the measles vaccine has now been found in the bowel of many children affected with autism and bowel disease, and d) the same vaccine strain has been found in the fluid surrounding the brain of some of these children and e) that thousands of parents with autism that started following the vaccine are convinced means that concerns aren’t likely to fade away. For example, in one UK survey of 825 parents whose children had symptoms that would classify them as autistic, 55 reported clear signs of regression following the MMR vaccine.
There’s a simple solution if measles is the primary concern, and that is to bring back the option of the much more effective and safer single measles vaccine which has not been associated with triggering autism. Why not? There is nothing to lose by doing this. Alternatively, there is a case of just accepting that total measles eradication, a non-life threatening infection provided a child isn’t malnourished with vitamin A deficiency, isn’t going to happen. Getting measles as a child confers life-long immunity which vaccination does not.
As for the HPV vaccine the big resistance relates to the undeniable risk of serious auto-immune diseases that have occurred in now well over a thousand girls following the HPV vaccine, quite apart from suspected deaths. The current conservative estimate is that a girl is 40 times more likely to have a serious auto-immune reaction that may not resolve than to die from cervical cancer, which, if caught early never need cause death.
If the MMR and HPV vaccine had not clearly been linked to inducing irresolvable reactions that have ruined children’s and young girl’s lives I’m sure the vaccine uptake would be higher. Until these adverse reactions are properly researched in order to create safer vaccines, rather than being flatly denied and swept under the rug, some people will understandably be resistant to exposing their child to that risk. That does not make them ‘morally reprehensible, deeply irresponsible’ nor an anti-vaxxer. It makes them a concerned parent. I do not consider myself to be an anti-vaxxer but nor am I a vaccine damage denier. Compulsory vaccination is not the answer. It is just bullying and crosses an ethical line of enforcing medication. It is morally reprehensible unless there is a genuine medical emergency which, clearly, there is not.
Vaccines – EXPLORING THE ISSUES
If you’d like to read more about vaccines – which ones are needed and which ones have the most safety concerns and how to mitigate risk – it is all covered in my November newsletter for 100% Health Club Members.
Vaccines is almost a taboo subject, thanks to the brilliant media campaign targeting anti-vaxxers as health terrorists. Even the Guardian said “While we fret about rising sea levels …. the threat posed by Russia …a lunatic in the White House…. it’s going to be the anti-vaxxers who end up killing all of us.” Against this hysteria I thought it worth dedicating this month’s newsletter to look at the important health questions that are not being addressed in this climate of polarities. Firstly, to make it clear, I am not an anti-vaxxer, in the same way I’m not anti all drugs. Some work well, some don’t, some have a questionable benefit/risk ratio and, as we’ve learnt from the last few decades of watching the pharmaceutical industry, some are over-sold for profitable reasons, with downsides downplayed as much as possible. I’m also not a vaccine damage denier. Vaccines, like any health treatment, need to be open to proper scientific evaluation regarding their benefit versus risk.
There’s a lot of new vaccines being added to the schedule for children that have not been properly evaluated, and are of dubious benefit. The new Hepatitis B vaccine is an example. It affects less than ten children a year, transmitted by sex and blood. Even more worrying is talk of compulsory vaccines. Making any treatment compulsory is an appropriate if there’s an emergency. There isn’t one. Take measles. The annual death rate is between one and zero for the past 20 years.
Yet Germany has drafted a law to fine a parent €2,500 if they don’t have the MMR jab. Matt Hancock, the new Health Secretary, has said he’s considering making childhood vaccines mandatory to achieve ‘herd’ immunity. This figure is usually estimated at around 95% vaccinated, but the MMR is much less than 95% effective, and less effective for measles than a single vaccine, which many parents rightly wary of the MMR, want. Often, in measles and mumps outbreaks, a high percentage of vaccinated children get the illness. So, even 100% vaccinated wouldn’t achieve this, if it is desirable. There is an argument that it is much better to get measles and mumps when you’re young, conferring lifetime immunity. The MMR doesn’t do this. The mumps component is 65% effective after one dose, and 88% effective after two, according to a study of a mumps outbreak in the Journal of Pediatrics.
Similarly, deaths from cervical cancer, which should never kill if caught early, is not on the increase. With 870 deaths a year that’s a one in 37,037 risk, compared with the conservative risk of a serious adverse reaction to the vaccine of one in 1,757. One drug company funded study reported nine cases of auto-immune disease in 9,000 vaccinated. This means that a girl is 21 times more likely to have a serious adverse reaction from the vaccine than to die from cervical cancer, but that assumes the vaccine is 100% effective at preventing cervical cancer. If only 50% effective (which is an optimistic figure – there are many strains of the human papilloma virus (HPV). One recent study reported 46% effectiveness at stopping high grade cervical abnormalities, not cancer, in those who had had three doses. Another 20% less chance of infection with at least one vaccine dose – see full article for refs.) then a girl is 40 times more likely to get a serious adverse reaction than to die from a sexually transmitted disease which is, in any event, largely preventable by safe sex and not being too promiscuous, keeping an eye out for genital warts and lumps, and cervical smears. Why are we not having this kind of informed debate? Proposals to extend HPV vaccine to boys has no basis in scientific logic, even according to the World Health Organisation, who tend to be pro-vaccines.The issues I’m interested in are:
- The flu jab – how effective is it? Are there any downsides and anything that works better?
- HPV vaccination – should all teenage boys and girls have it?
- MMR – that old chestnut. What have we learnt? Almost a quarter of children in some areas haven’t had it.
- Aluminium – it’s in most vaccines specifically to get the immune system to attack the invading pathogen. We are told it’s in tiny amounts and is, anyway, harmless. Is this true?
- Multiple vaccines – as more and more vaccines are added to the schedule a child is meant to receive is there any danger that occurs with multiple vaccines?
- What does a child actually need in the way of a vaccine schedule
A vaccine damage denier would just deny any problems but this cannot be so. In the US, but sadly not in the UK, there’s a relatively simple, and transparent way of reporting an adverse reaction to a vaccine. Anyone can see the list for themselves, broken down by vaccine and by symptom at https://vaers.hhs.gov. This year, for example, there have been over 24,000 adverse reactions reported by mid August. Many of these are minor, and resolve. Some are extremely crippling and persist. Two new syndromes linked to the HPV vaccine are complex regional pain syndrome (CRPS) and postural orthostatic tachycardia syndrome (POTS). As of May 2018, the WHO UMC VigiBase had identified 526 cases of POTS and 168 cases of CRPS reported related to HPV vaccination. Bearing in mind that an estimated 1 to 10% of adverse reactions are reported the actual number of cases will be higher. Also, hundreds of millions of pounds a year are paid out by the American government compensation scheme for vaccination injuries. Part way through 2017, the Health Resources and Services Administration had paid out over 142 million dollars for cases settled so far that year. So side effects are not negligible. That’s why you have to look at the risk versus the benefit.
Some hold steadily to the maxim of herd immunity – that everyone must have the vaccine to wipe out the disease to protect the more vulnerable. But this doesn’t apply to some infectious agents which rapidly mutate to survive. There’s even evidence that this might be happening to measles. Human flu strains are also always changing which is why herd immunity is not possible and why the success rate of flu jabs is not so high – only 10% effective in over 60 year olds last year. Should everyone take antibiotics to wipe out certain bacterial pathogens? We have learnt that this way of thinking has actually created more superbugs, no longer responsive to existing antibiotics. We could be heading the same way with over-vaccination. Thus, the concept of strengthening the host, not just killing the invader, is the other side of the coin worthy of consideration but rarely discussed since drugs and vaccines don’t do this, however good nutrition can. Vitamin A and vitamin CWhat it does: Strengthens immune system – fights infections. Makes collagen, keeping bones, skin and joints firm and strong. Antioxidant, detoxifying pollutants and protecting against… both help measles become a minor affair.
These, and other issues, will be explored in my November newsletter. If you’re interested make sure your 100% Health Club membership is up to date.
Comments
Join the Conversation on our Facebook Page